584 - Sedation/Anesthesia Use for Inpatient Pediatric Brain MRIs: National Trends and Outcomes
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2569.584
Chloë Nunneley, University of Texas Southwestern Medical School, Dallas, TX, United States; Matt hall, Children's Hospital Association, Lenexa, KS, United States; Stephanie B. Arar, University of Texas Southwestern Medical School, Dallas, TX, United States; Kristen Calhoun, University of Texas Southwestern Medical School, Dallas, TX, United States; Whitney Cameron, University of Texas Southwestern Medical School, Dallas, TX, United States; William C. Hancock, University of Texas Southwestern Medical School, Bedford, TX, United States; Andrew Yu, University of Texas Southwestern Medical School, Dallas, TX, United States
Assistant Professor University of Texas Southwestern Medical School Dallas, Texas, United States
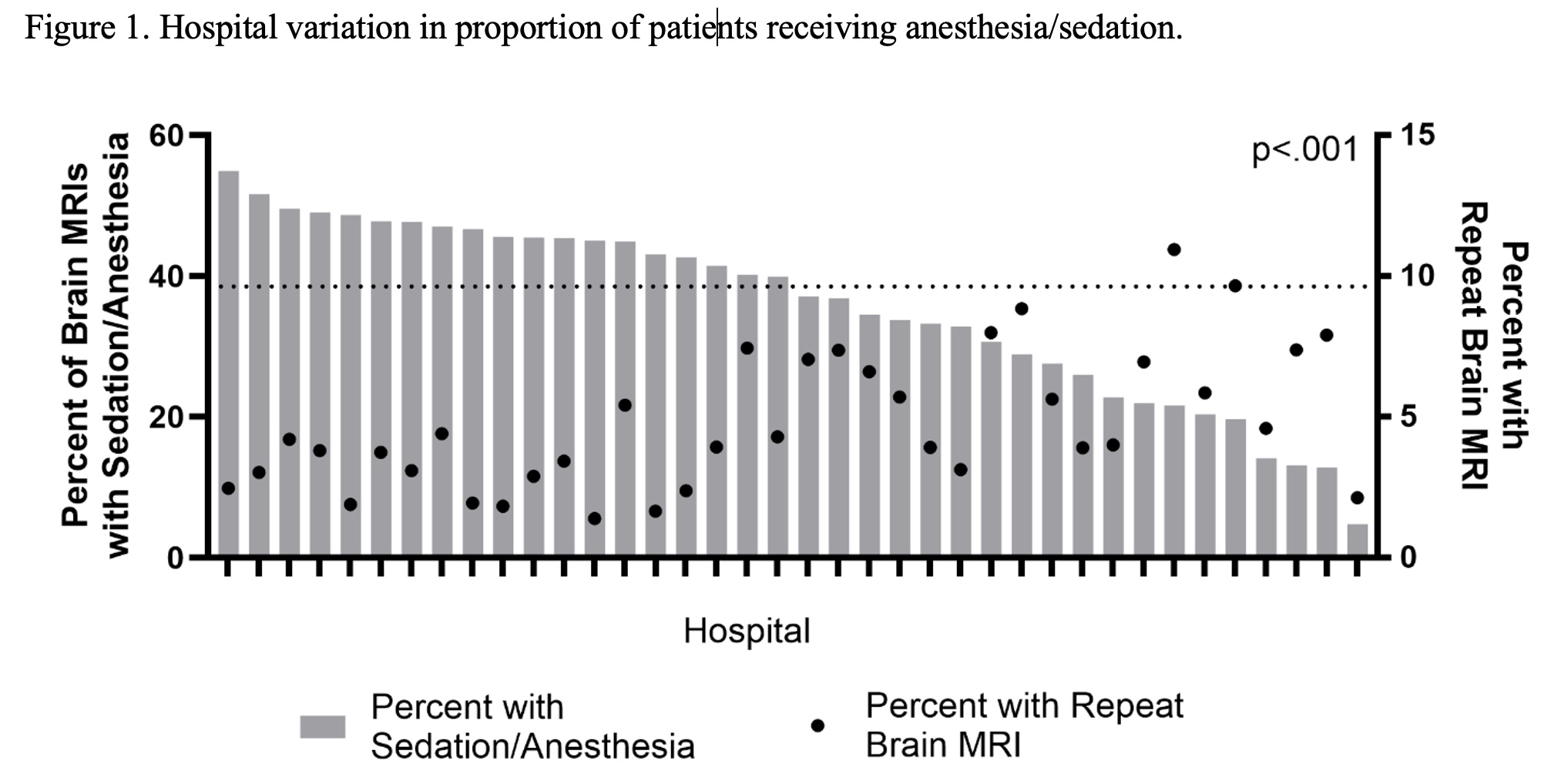
Background: Brain magnetic resonance imaging (MRI) is the most common MRI acquired in children's hospitals. Sedation/anesthesia may be utilized in pediatric patients to obtain adequate image quality; however, it may be associated with future neurocognitive deficits and incurs significant cost. While reducing overuse of sedation/anesthesia has been identified as an area of improvement, national studies describing trends in sedation/anesthesia utilization, hospital variation, and outcomes in hospitalized children undergoing brain MRI are lacking. Objective: To understand trends, patient demographics, hospital variation, and clinical outcomes associated with sedation/anesthesia for pediatric brain MRIs. Design/Methods: This retrospective cohort study utilized Pediatric Health Information System data for children < 18 years old that received an inpatient brain MRI from 2014-2024. Outcomes included the need for a repeat brain MRI, length of stay (in days), cost, and mortality. The likelihood of receiving sedation/anesthesia was modeled using Generalized Estimating Equations (GEE), clustered on hospital and adjusted for important clinical and demographic factors. Outcomes were also modeled using GEEs to compare those with and without sedation/anesthesia. Results: Of 215,377 index brain MRIs, 36.4% utilized sedation/anesthesia. Sedation/anesthesia use peaked in early childhood and was more common among patients with mental health diagnoses, but less common among patients with multiple complex chronic conditions (Table 1). Compared to no sedation/anesthesia, the use of sedation/anesthesia was associated with a lower likelihood of repeat MRI (aOR 0.29, 95% CI: 0.25-0.34) and higher cost (aRR 1.27, 95% CI: 1.13-1.42); there were no meaningful differences in LOS or mortality (Table 2). There was significant hospital to hospital variation in the use of sedation/anesthesia, ranging from 4.8% to 54.9% (Figure 1).
Conclusion(s): We found that a significant proportion of pediatric brain MRIs are being obtained with sedation/anesthesia, with highly variable rates across hospitals. Among children undergoing brain MRI, the rate of repeat imaging was low, even for children who do not receive sedation/anesthesia, and LOS is similar. Given the neurocognitive risk and high cost associated with sedation/anesthesia, both provider-level and institutional-level initiatives could be impactful in reducing unnecessary sedation/anesthesia among pediatric patients.
Table 1. Demographic and clinical characteristics of hospitalized children that had a brain MRI, stratified by receipt of sedation/anesthesia Table 1.pdf
Table 2. Adjusted outcomes based on utilization of sedation/anesthesia. Table 2.pdf
Figure 1. Hospital variation in proportion of patients receiving anesthesia/sedation.

 photo")