601 - Screening While Admitted: Increasing Sexually Transmitted Infection Screening Rates in Adolescent Patients by Testing in the Inpatient Setting
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2586.601
Zainab Khan, University of California, San Diego School of Medicine, San Diego, CA, United States; Amy Z. Chong, UC San Diego/Rady Children's Health San Diego, San Diego, CA, United States; Tatyana G. Mills, University of California, San Diego School of Medicine, San Diego, CA, United States; Heather Pierce, Rady Children's Hospital San Diego, San Diego, CA, United States
Pediatric Hospital Medicine Fellow University of California, San Diego School of Medicine San Diego, California, United States
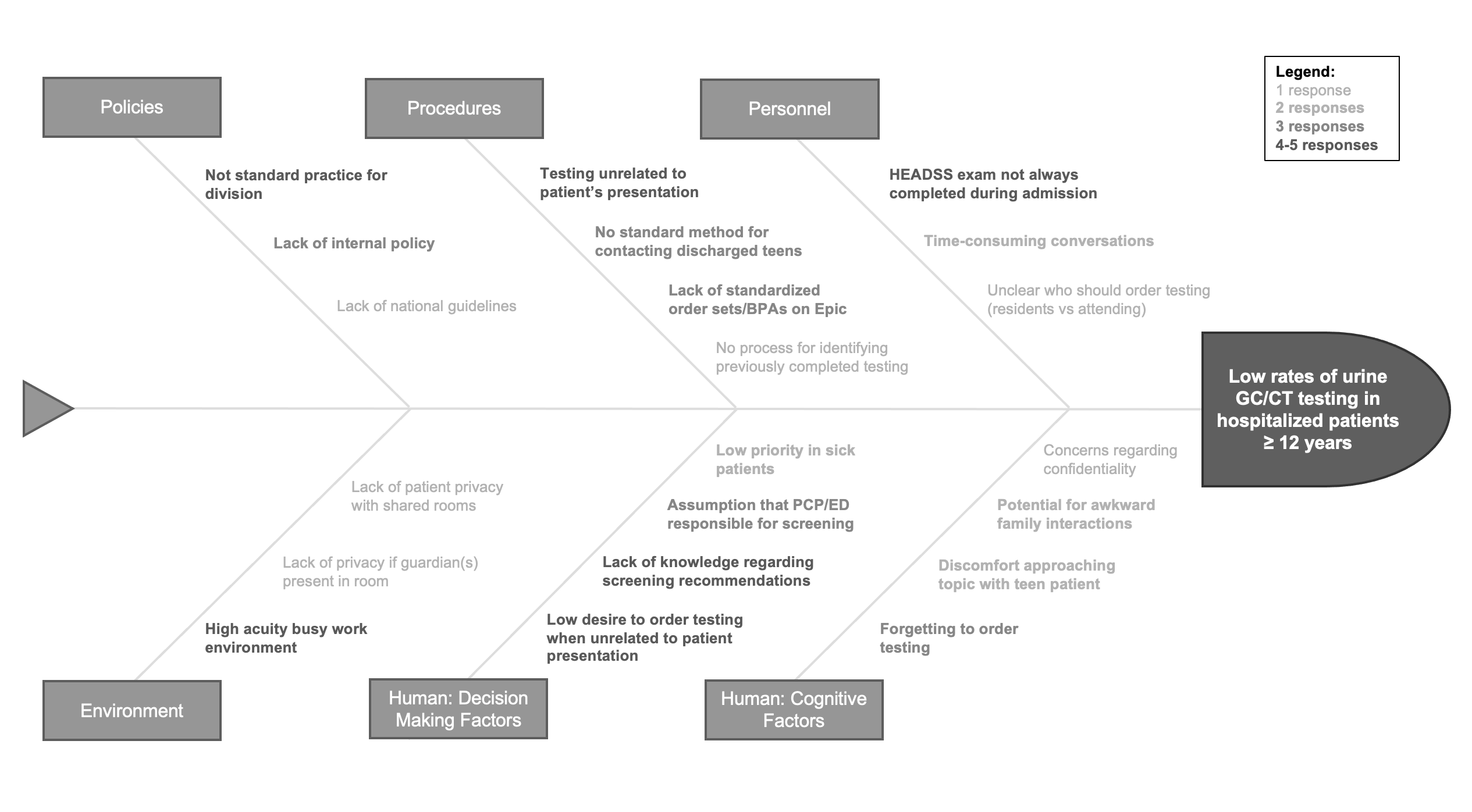
Background: Adolescents and young adults acquire nearly 50% of all new sexually transmitted illnesses (STIs) per year; however, they face numerous barriers to receiving appropriate care including low healthcare utilization, confidentiality concerns, and lack of knowledge of STIs. Objective: To increase the percentage of gonorrhea and chlamydia screening in patients ≥ 12 years without diminished capacity and without screening in the prior 60 days admitted to pediatric hospital medicine (PHM) service from 22% to 50% in 12 months. Design/Methods: In this IRB-exempt QI study, we used QI methodology with a multidisciplinary team to achieve our aims. Ishikawa and key driver diagrams identified barriers and drivers to improving screening rates (Figures 1 and 2). A baseline rate of 22% (1-8/2024) was obtained via electronic health record (EHR) review. Interventions included faculty education (9/2024), adolescent contact preference workflow, provider/nurse scripts, and treatment algorithm (10/2024), twice weekly EHR active chat reminders (12/2024), H&P template modifications with in-line rule-based clinical decision support (CDS) (1/2025), and an order set-based CDS tool (2/2025). The primary outcome measure was the percentage of eligible patients undergoing gonorrhea and chlamydia screening with secondary outcome measures including number of positive results and number of patients with positive results receiving appropriate treatment. Our process measure was utilization of CDS tool, and the balancing measures were breach of confidentiality and dissatisfaction with testing. Results: The implementation of faculty education, contact preference workflow, provider/nurse scripts, and treatment algorithm preceded a center line shift to 42% (Figure 3). After the implementation of the H&P template changes and the order set-based CDS tool, special cause variation was seen with another center line shift to 80%. We surpassed our target of 50% screening rate. Further data is ongoing for sustainability. Among those screened, 5 patients tested positive for chlamydia; all received appropriate treatment. There were no reports of breach of confidentiality or dissatisfaction with testing.
Conclusion(s): This PDSA-driven project increased STI screening in adolescents with a centerline shift from 22% to 80% in 12 months. All identified cases were treated. The biggest gains came after implementation of the CDS tools, demonstrating that EHR-based strategies can effectively boost and sustain screening rates.

 Credit")
 photo")
.png)
.png)
