43 - Body composition indicators to identify nutritional risk at NICU discharge: comparison with anthropometry based classification
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2040.43
Katherine A. Bell, Harvard Medical School, Boston, MA, United States; Wei Wang, Brigham and Women's Hospital, Boston, MA, United States; Emily M. Nagel, University of Minnesota Department of Pediatrics, Minneapolis, MN, United States; Erin Plummer, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Hunter L. Pepin, Brigham and Women's Hospital, Boston, MA, United States; Sara E. Ramel, University of Minnesota Masonic Children's Hospital, North Oaks, MN, United States; Mandy Belfort, Harvard Medical School, Boston, MA, United States
Assistant Professor Brigham and Women’s Hospital Boston, Massachusetts, United States
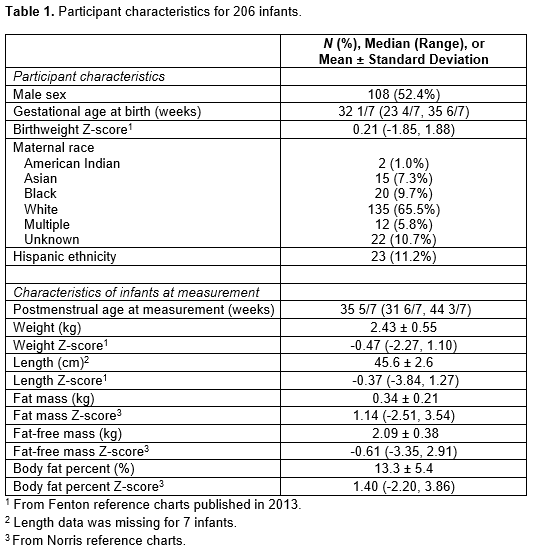
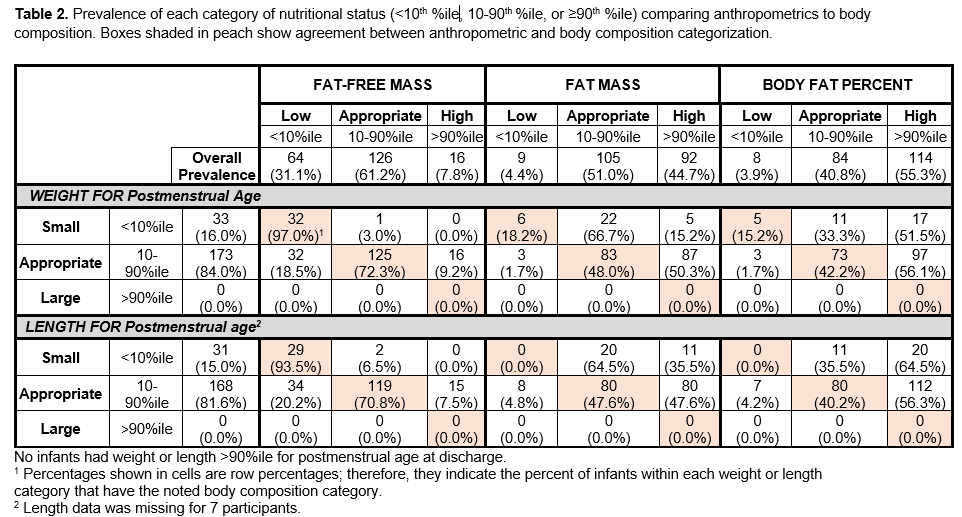
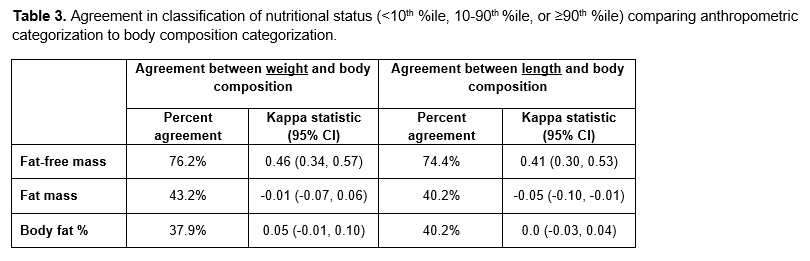
Background: Body composition is an emerging nutritional status indicator among preterm infants and may be more sensitive than anthropometrics (weight, length) for predicting health and developmental outcomes. Specifically, low fat-free mass is associated with poorer neurodevelopment and excess fat may predict metabolic risk. Yet, the extent to which classification of nutritional status by body composition differs from classification based on weight and length remains unknown. Objective: Among preterm infants at or near term equivalent age, to determine agreement between categorization of size by weight or length and categorization of size using body composition. Design/Methods: Singleton preterm infants ( < 36 weeks' gestation [GA]) enrolled in the BabyBEAN multi-center observational study were measured near or at term equivalent age with air displacement plethysmography (ADP) to determine fat-free mass (FFM), fat mass (FM), and body fat percent (%FM), which we converted to Z-scores using the Norris ADP reference. Concurrently measured weight and length were converted to Z-scores using Fenton charts from 2013. All Z-scores were categorized as low ( < 10th percentile), appropriate (10- < 90th percentile), or high (≥90th percentile). Agreement between weight or length Z-score category and body composition Z-score category was quantified by percent agreement and kappa (κ) statistic. Results: 206 infants with median GA 32 1/7 (range 23 4/7, 35 6/7) weeks were measured at median PMA 35 5/7 (range 31 6/7, 44 3/7) (Table 1). The prevalence of weight < 10%ile was 16.0% and of length < 10%ile was 15.0%. Low FFM < 10%ile was more common and occurred in 31.1% of infants, and high FM >90%ile in 44.7% (Table 2). Among 173 infants categorized as having appropriate weight Z-score, low FFM occurred in 32 (18.5%) and high FM in 83 (48.0%). There was moderate agreement of anthropometric categorization with FFM categorization; percent agreement for weight and FFM was 76.2% and κ=0.46 (95% CI: 0.34, 0.57). Agreement of anthropometrics with fat categorization was poor (percent agreement 37.9%-43.2%, κ ranging -0.05 to 0.05) (Table 3).
Conclusion(s): Weight and length alone do not identify all preterm infants with low FFM or excess adiposity. Therefore, body composition measurement provides valuable information about growth and nutrition-related risks that cannot be determined from simple anthropometrics alone. Our findings support the clinical utility of body composition measurement for preterm infants.

 photo")