628 - Hemodynamic Effects of Milking the Cut-Cord in Very Preterm Infants: A Randomized Controlled Trial (Hemodynamics of MoCC Trial)
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2613.628
Walid El-Naggar, Dalhousie University, Halifax, NS, Canada; Souvik Mitra, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Jayani Abeysekera, Dalhousie University Faculty of Medicine, Halifax, NS, Canada; Tim Disher, IWK Health Centre, West Porters Lake, NS, Canada; Tara R. Hatfield, IWK Health, Halifax, NS, Canada; Ahmed Galal, Dalhousie University, Halifax, NS, Canada; Christy G. Woolcott, Dalhousie University Faculty of Medicine, Halifax, NS, Canada; Jon Dorling, University of Leeds, Leeds, England, United Kingdom
Professor of Pediatrics Dalhousie University Halifax, Nova Scotia, Canada
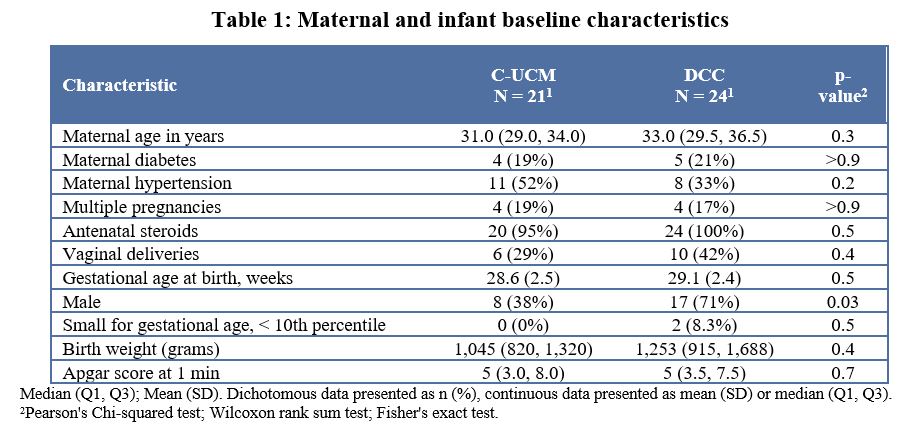
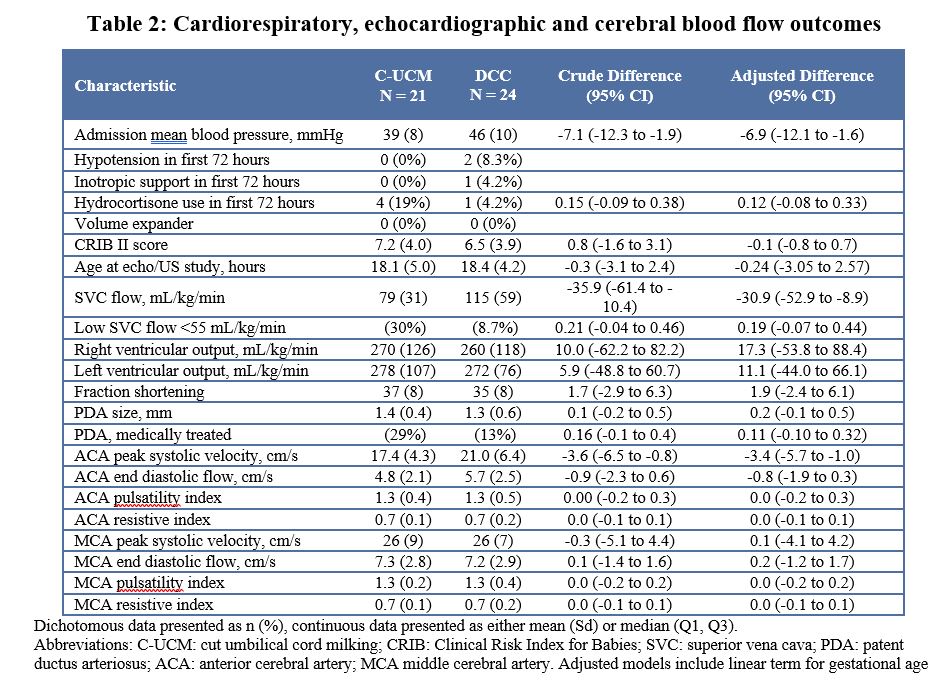
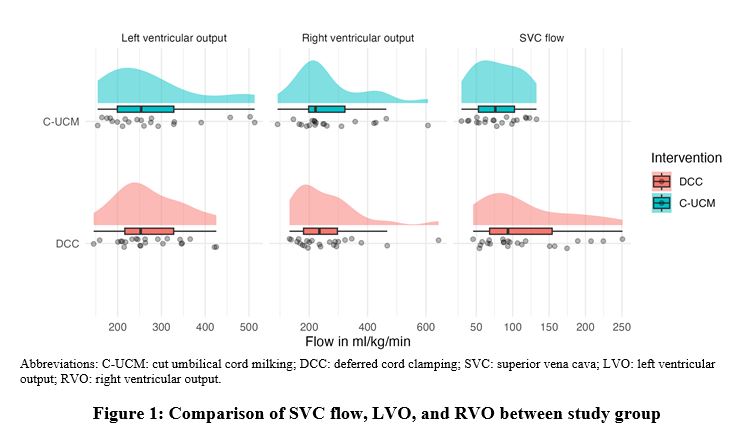
Background: Cut-umbilical cord milking (C-UCM) may be an alternative when deferred cord clamping (DCC) is not feasible. Earlier, we reported the feasibility of C-UCM in very preterm infants. Objective: To investigate hemodynamic effects of C-UCM during stabilization of very preterm infants after birth. Design/Methods: In this sub-study of the MoCC trial, infants born to eligible, consenting women presenting in labor at < 32 weeks' gestation were randomized to C-UCM while supporting breathing following 30 seconds of DCC (to provide initial resuscitation steps) or DCC for 30-60 seconds (standard practice). Clinical, echocardiographic and cerebral blood flow measures (at 12-24 hours of age) were compared between both groups. The ultrasonographer and interpreter were blind to randomization. Analysis was by intention to treat. Results: Forty-five infants (C-UCM, n=21; DCC, n=24) received full hemodynamic assessment. Mean gestational age (SD) was 28.8 (2.4) weeks (Table 1). Mean blood pressure on admission and SVC flow at 12-24 hours were lower in the C-UCM group [adjusted mean difference (95% CI) -6.9 mmHg (-12.1, -1.6) and -30.9 mL/kg/min (-52.9, -8.9), respectively (Table 2). However, the risks of hypotension in the first 72 hours and low SVC flow < 55 mL/kg/min were not significantly different. Similarly, measures of left ventricular function, cardiac output, and cerebral blood flow were not significantly different between the groups.
Conclusion(s): C-UCM after 30 seconds of DCC and while supporting breathing, may not cause hemodynamic compromise compared to the standard practice of DCC for 30-60 seconds. These findings support the feasibility of C-UCM in very preterm infants.
Table 1: Maternal and infant baseline characteristics
Table 2: Cardiorespiratory, echocardiographic and cerebral blood flow outcomes
Figure 1 Comparison of SVC flow, LVO, and RVO between study group