208 - Identifying Suicide Risk Factors Among Rural-Residing Youth: Perspectives of Community Members in Northern New England
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2200.208
Emma R. Jacobs, Geisel School of Medicine at Dartmouth, Lebanon, NH, United States; Jacqueline A. Pogue, The Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH, United States; Nikolas G. Hernandez, Geisel School of Medicine at Dartmouth, White River Junction, VT, United States; Alyssa C. Helmling, Geisel School of Medicine at Dartmouth, Lebanon, NH, United States; Stephanie C. Acquilano, Geisel School of Medicine at Dartmouth, Lebanon, NH, United States; Christine Finn, Geisel School of Medicine at Dartmouth, Lebanon, NH, United States; Alison Kapadia, Geisel School of Medicine at Dartmouth, Lebanon, NH, United States; Maia Rutman, Children's Hospital at Dartmouth-Hitchcock, Lebanon, NH, United States; JoAnna Leyenaar, The Dartmouth Institute of Health Policy & Clinical Practie, Lebanon, NH, United States
Medical Student Geisel School of Medicine at Dartmouth Lebanon, New Hampshire, United States
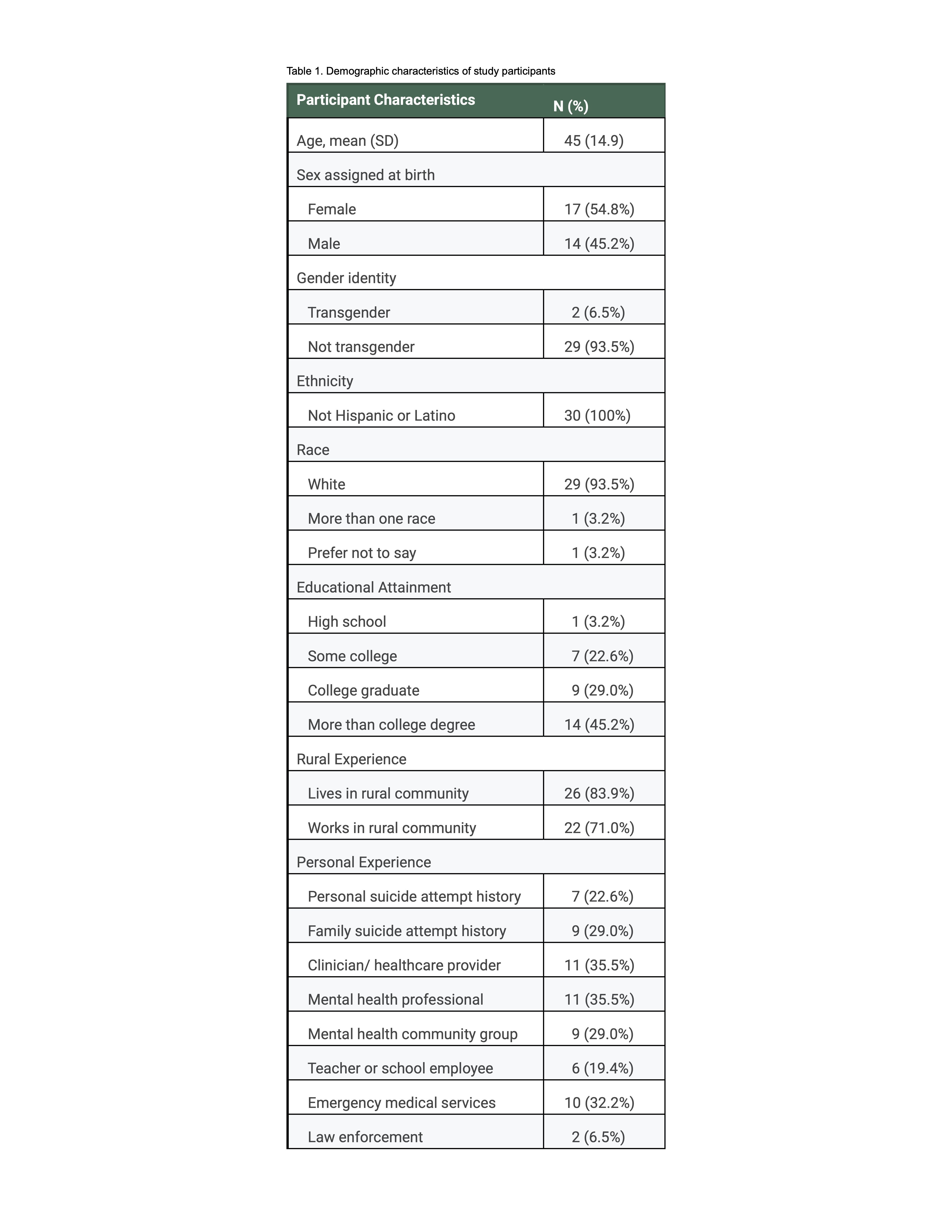
Background: One in five adolescents in the US live in rural communities, where suicide rates among youth are twice those of urban areas. However, the unique cultural, environmental, and structural factors contributing to this elevated risk remain poorly understood. Objective: To explore unique suicide risk factors and barriers to prevention for adolescents from the perspectives of rural-residing residents in Northern New England. Design/Methods: Between March and April 2025, six focus groups and five individual interviews were held virtually via video-conference with 31 residents of rural New Hampshire and Vermont. Questions focused on: (i) unique adolescent suicide risks in rural communities, (ii) firearm and medication safety, and (iii) barriers to mental health care access. Sessions were audio-recorded, transcribed, and analyzed using practical thematic analysis. Results: Participants held multiple roles, including clinicians, mental health professionals, individuals with personal or family history of suicide attempt, mental health community group members, school personnel, and law enforcement (Table 1). Participants identified several suicide risk factors and barriers to prevention in rural settings (Table 2). Cultural factors included fatalistic attitudes toward suicide, minimization of suicide incidence, and firearm ownership culture that emphasized gun safety for injury prevention but rarely addressed suicide prevention. While firearm safety training was common, early exposure and multigenerational cultural ties created resistance to lethal means restriction. Medication risks were amplified by rural-specific factors: larger home supplies due to limited pharmacy access and multigenerational households, safe storage challenges, and underappreciation of over-the-counter medication dangers. Structural barriers compounded risk through geographic and social isolation that limited peer connections, increased substance use, and heightened reliance on online interactions. Critically, insufficient mental health resources have impeded engagement in safety planning. Participants also noted environmental hazards unique to rural settings, including exposure to natural elements and access to open water.
Conclusion(s): Perceptions of rural youth suicide risk are shaped by local cultural norms and experiences. These findings can be used to inform clinical care of children and families in rural communities as well as public health efforts to reduce youth suicide risk.
Table 1. Demographic characteristics of study participants
Table 2. Emerging themes and representative quotes summarizing rural-residing community members' perspectives on rural youth suicide risks

 photo")
.png)
