568 - Examining routine daily chest radiograph use for children hospitalized with parapneumonic effusions requiring chest tube placement
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2553.568
Christiane Lenzen, University of California, San Diego School of Medicine, San Diego, CA, United States; Elizabeth Mannino Avila, UCSD/Rady Children's Hospital San Diego, San Diego, CA, United States; Melissa Cameron, Rady Children's Hospital San Diego, San, CA, United States; Kyung E.. Rhee, UC San Diego School of Medicine, LA JOLLA, CA, United States; Michelle Polich, University of California, San Diego, San Diego, CA, United States
Associate Professor of Pediatrics University of California, San Diego School of Medicine San Diego, California, United States
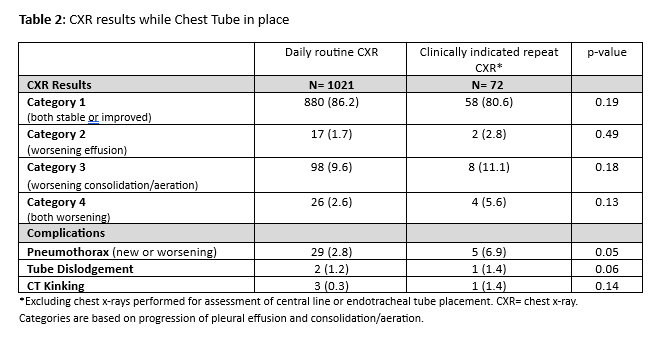
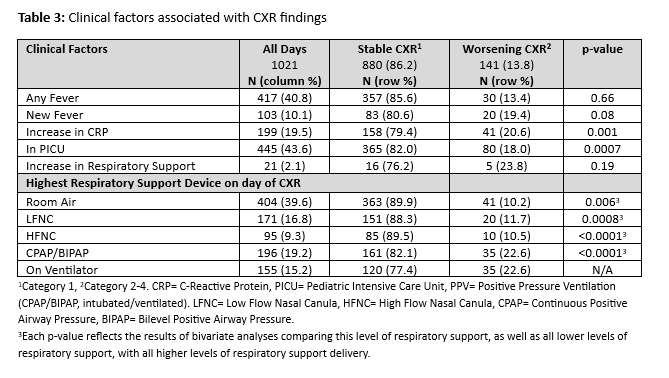
Background: Children with pneumonia complicated by parapneumonic effusion often require chest tubes (CT). Daily routine chest x-ray (DR-CXR) to monitor CT complications is a common practice, but the clinical value of these CXRs has not been systematically studied. Objective: The goal of this study was to 1) determine the frequency of complications found on DR-CXRs for hospitalized children with a CT secondary to complicated pneumonia and 2) identify clinical characteristics associated with worsening DR-CXR findings. Design/Methods: We conducted a retrospective chart review at a large free-standing Children's Hospital including hospitalized children 6 months-18 years with a CT for bacterial pneumonia with effusion from 10/2016 to 9/2024. Findings on DR-CXRs after CT placement were classified into 4 categories based on progression of effusion and consolidation/aeration: 1) both stable/improved, 2) worsening effusion, 3) worsening consolidation/aeration, 4) worsening of both. In addition, complications of kinking, CT dislodgement, and pneumothorax were noted. Clinical characteristics associated with worsening condition included: fever, CRP, respiratory support and transfer to intensive care unit. Mixed-effects logistic regression model, accounting for repeated daily observations and including covariates was used to determine clinical factors associations with stable DR-CXR findings. Results: There were 169 patient encounters with a median of 5.0 [IQR 4.0-7.0] days following CT placement until removal or secondary CT placement (Table 1). Out of a total of 1041 days, 1021 days (98%) had a DR-CXR performed. Most (86%) were stable or improved. The most common complication on these DR-CXRs was pneumothorax (n=29, 2.8%) and of these only 3 had secondary CT placement. Other complications include tube dislodgement (1.2%) and tube kinking (0.3%) (Table 2). On 191 days (19%), repeat imaging of any kind (CXR, ultrasound, computer tomography) was obtained for clinical indication, and CXRs were obtained on 72 of these days. After adjusting for covariates, daily clinical factors associated with a stable DR-CXR included no CRP increase (OR 1.64, 95% CI 1.06-2.52) and not being on positive pressure ventilation (OR 2.05, 95% CI 1.38-3.05) (Table 3).
Conclusion(s): DR-CXRs in pediatric patients with a CT for complicated pneumonia rarely found worsening consolidation, aeration, or effusion. Detection of complications was very low and rarely resulted in placement of a second chest tube. Further studies should examine use of DR-CXR versus targeted imaging and further deepen understanding of clinical indicators to guide practice patterns.
Table 1: Demographics and Characteristics of Study Population (Patient Encounter Level)
Table 2: CXR results while Chest Tube in place
Table 3: Clinical factors associated with CXR findings

 photo")
.png)