526 - Racial and Ethnic Disparities in High Flow Nasal Cannula Use in Bronchiolitis
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2511.526
Shrushti Mehta, Children's Hospital of Michigan, Warren, MI, United States; Robert Ehrman, Wayne State University School of Medicine, Detroit, MI, United States; Amber Gasparini, Children's Hospital of Michigan, Farmington Hills, MI, United States; Caitlyn Thornbury, Central Michigan University College of Medicine, Mount Pleasant, MI, United States; James McConnell, Central Michigan University College of Medicine, Bay City, MI, United States; Karen Crile, Central Michigan University College of Medicine, Detroit, MI, United States; Anusha R. Desai, Central Michigan University College of Medicine, Mount Pleasant, MI, United States; Bhumi Patel, Central Michigan University College of Medicine, Troy, MI, United States; NIrupama Kannikeswaran, Central Michigan University, Children's Hospital of Michigan, Detroit, MI, United States
Pediatric Emergency Medicine Fellow Children's Hospital of Michigan Warren, Michigan, United States
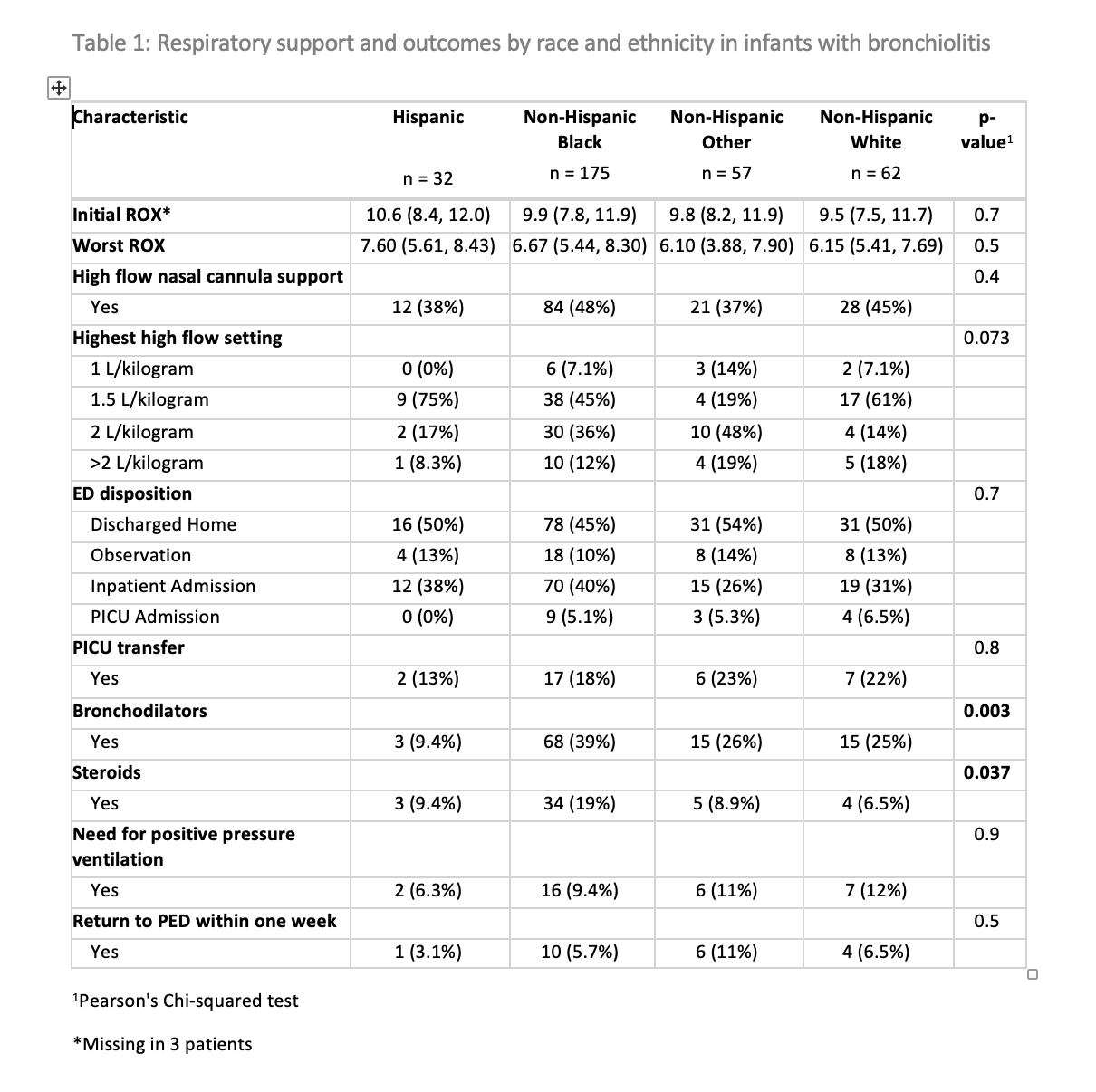
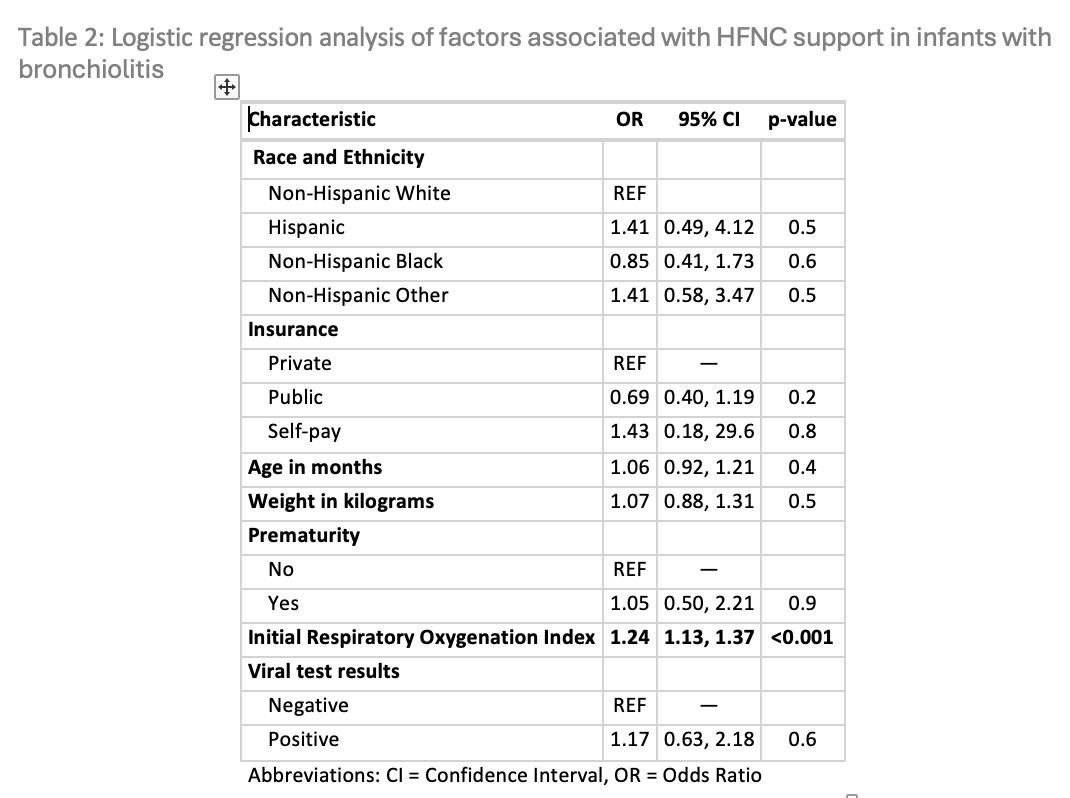
Background: Use of high-flow nasal cannula (HFNC) for respiratory support in infants with bronchiolitis has increased significantly in recent years. Although racial and ethnic disparities exist in adherence to evidence-based bronchiolitis management, few studies have examined whether such differences occur in HFNC use. Objective: To assess if racial and ethnic disparities exist in HFNC use in infants with bronchiolitis. Design/Methods: We conducted a retrospective study of infants ≤12 months with bronchiolitis who presented to an inner-city, level I pediatric emergency department between January 2023 and January 2025. Patients were identified using ICD-10 codes (J21.0, J21.1, J21.8, J21.9) for diagnosis of bronchiolitis. Data collected included demographics, prematurity, respiratory oxygenation index (ROX; initial and worst values), type of respiratory support, bronchodilator and steroid use, disposition, and return visits. Race and ethnicity were categorized as non-Hispanic White (NHW), non-Hispanic Black (NHB), non-Hispanic Other (NHO), and Hispanic. The primary predictor was race and ethnicity, and the primary outcome was HFNC use. Logistic regression was used to evaluate the association between race and ethnicity and HFNC use, adjusting for age, weight, prematurity, insurance, ROX, and viral testing. Results: Among 326 patients, the majority were male (n = 201; 62%) with a median age of 5 months (IQR 2.0-8.0) and median weight of 7.6 kg (IQR 5.79-8.64). Fifty-two patients (16%) had a history of prematurity. Racial and ethnic distribution was as follows: NHW (n = 62; 19%), NHB (n = 175; 54%), NHO (n = 57; 17%), and Hispanic (n = 32; 9.8%). Nearly half were admitted (n = 154; 48%), and 16 (4.9%) required intensive care. HFNC was initiated in 145 patients (44%). HFNC use, need for positive pressure ventilation, and return visits did not differ by race or ethnicity. However, bronchodilator use was less common among Hispanic patients, and NHB patients were more likely to receive steroids (Table 1). Logistic regression showed no association between race and ethnicity and HFNC use; only initial ROX was independently associated with HFNC use (Table 2).
Conclusion(s): In this single-center study of infants with bronchiolitis, HFNC use did not differ by race or ethnicity after adjusting for demographic and clinical factors. However, there were disparities in bronchodilator and steroid use. These findings highlight the need to further examine treatment variations to ensure equitable, evidence-based care in bronchiolitis.
Table 1: Respiratory support and outcomes by race and ethnicity in infants with bronchiolitis
Table 2: Logistic regression analysis of factors associated with HFNC support in infants with bronchiolitis