530 - Sizing Up Septic Arthritis: Diagnostic Utility of Ultrasound Measurements of Pediatric Hip Effusions
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2515.530
Antonio Riera, Yale University, New Haven, CT, United States; Laurie Malia, Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States; Margaret Rinaldi, Medical University of South Carolina, Charleston, SC, United States; Ruchika M. Jones, Connecticut Children's Medical Center, Hartford, CT, United States; Ee Tein. Tay, NYU Langone Health, New York, NY, United States; Maytal Firnberg, UCSF Benioff Children's Hospital San Francisco, San Francisco, CA, United States; William Mak, Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Flushing, NY, United States; Matthew Moake, Medical University of South Carolina, Charleston, SC, United States; Henry Chicaiza, Connecticut Children's, Suffield, CT, United States; Morgan T. Harper, Yale School of Medicine, Boston, MA, United States; Veronika Shabanova, Yale School of Medicine, New Haven, CT, United States; Peter J. Snelling, Gold Coast University Hospital, Gold Coast, Queensland, Australia
Associate Professor Yale University New Haven, Connecticut, United States
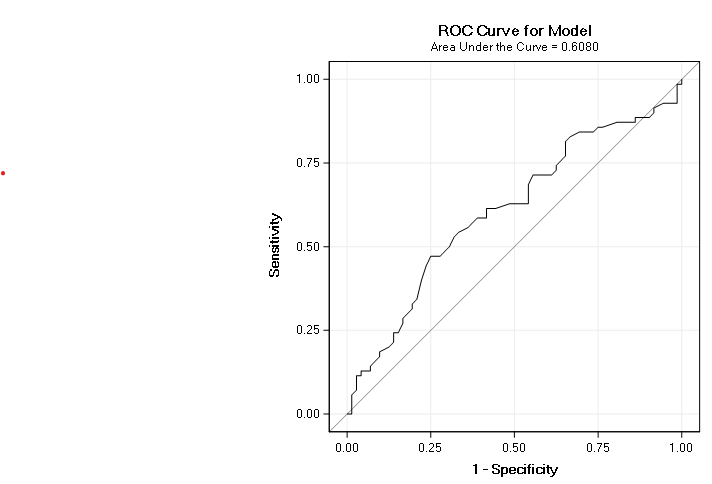
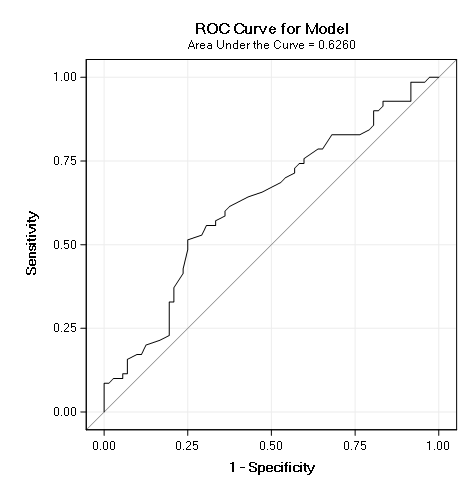
Background: Septic arthritis (SA) of the hip in children is a serious joint-threatening emergency requiring rapid diagnosis. Although ultrasound reliably detects hip effusions, its ability to distinguish SA from transient synovitis or Lyme arthritis remains uncertain. Objective: This study evaluates whether ultrasound characteristics of hip effusions can aid in differentiating SA from other causes of joint effusions in children. Design/Methods: We conducted a multicenter, retrospective case-control study of pediatric patients (≤18 years) presenting with limp who underwent hip ultrasound in a Pediatric Emergency Department from 2014-2024. Eligible patients had radiologist diagnosed hip effusions. SA cases were defined as patients requiring operative intervention with supportive microbiologic or clinical data. Controls were age, sex, and season-matched patients with alternative final diagnoses. Ultrasound images from eight sites in North America and Australia were reviewed by trained POCUS experts using a standardized protocol to measure the following distances across the widest aspect of the effusion: (1) anterior synovium-to-bone (ASB), (2) hypoechoic fluid pocket (HFP), and (3) anterior synovium thickness (AST). A novel effusion ratio (ER = HFP/ASB) was calculated to account for age-related capsular distention. Measurements were obtained from archived ultrasound images using hospital integrated imaging software. Receiver operator characteristic (ROC) curves with area under curve (AUC) for SA diagnosis were constructed from the ASB, HFP, AST, and ER measurements. Group comparisons used Fisher exact test for categorical variables and t-tests for continuous data. Results: A total of 70 patients with SA were identified across the 8 participating sites. Cases and controls were similar in age (mean 5.8 vs. 5.0 years, p=0.19), sex (46% vs. 42% female, p=0.63), weight (mean 23.9 vs. 22.0 kg, p=0.40), and effusion laterality (94% vs. 88% unilateral, p=0.19). ROC curve analysis demonstrated the following AUC values: ASB 0.61 (95% CI, 0.51-0.70), HFP 0.63 (95% CI, 0.53-0.72), AST 0.54 (95% CI, 0.45-0.64), and ER 0.59 (95% CI, 0.50-0.69). For the HFP measurement, the cutoff point with the highest Youden index was 6.5 mm, yielding a sensitivity of 51.4% and specificity of 75% to detect septic arthritis.
Conclusion(s): Ultrasound measurements of pediatric hip effusions including the overall size, the hypoechoic fluid component, and synovial thickness, demonstrated limited ability to distinguish septic arthritis from other causes. These preliminary findings should be validated in prospective studies.

 photo")
.png)
