644 - Therapeutic Hypothermia in Preterm Infants with Hypoxic-Ischemic Encephalopathy (HIE): A report from the Children's Hospitals Neonatal Consortium (CHNC) HIE Focus Group
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2628.644
Rakesh Rao, Washington University in St. Louis School of Medicine, St. Louis, MO, United States; Isabella Zaniletti, IZ Statistics LLC, Tampa, FL, United States; Vonita Chawla, Arkansas Children's Hospital, Little Rock, AR, United States; Jeffrey Shenberger, Connecticut Children's, Hartford, CT, United States; Mehmet Cizmeci, The Hospital for Sick Children, Toronto, ON, Canada; Robert DiGeronimo, Seattle Children's, Seattle, WA, United States; Katsuaki Kojima, Cincinnati Children's Hospital Medical Center, Montgomery, OH, United States; Karna Murthy, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Elizabeth Sewell, Emory University; Children's Healthcare of Atlanta, Atlanta, GA, United States; Ulrike Mietzsch, University of Washington School of Medicine/ Seattle Children's Hospital, Seattle, WA, United States; MIchael A. Padula, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Theresa Grover, Children's Hospital Colorado, Aurora, CO, United States; Ceyda Acun, Cleveland Clinic Children's Hospital, Cleveland, OH, United States; Jennifer A. Rumpel, University of Arkansas for Medical Sciences College of Medicine, Little Rock, AR, United States; Janessa Law, University of Washington School of Medicine, Seattle, WA, United States; Vilmaris Quinones Cardona, Drexel University College of Medicine, Philadelphia, PA, United States; Eric S. Peeples, University of Nebraska Medical Center, Omaha, NE, United States; Semsa Gogcu, Brown University, South Kingstown, RI, United States; Ryan M. McAdams, University of Wisconsin School of Medicine and Public Health, Middleton, WI, United States; Vikramaditya Dumpa, Arkansas Children's Hospital, Little Rock, AR, United States; Susan Cohen, CW HOPE Developmental Follow Up Clinic, Milwaukee, WI, United States; Maria L. V.. Dizon, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Girija Natarajan, Central Michigan University College of Medicine, Detroit, MI, United States
Associate Professor of Pediatrics Washington University in St. Louis School of Medicine St. Louis, Missouri, United States
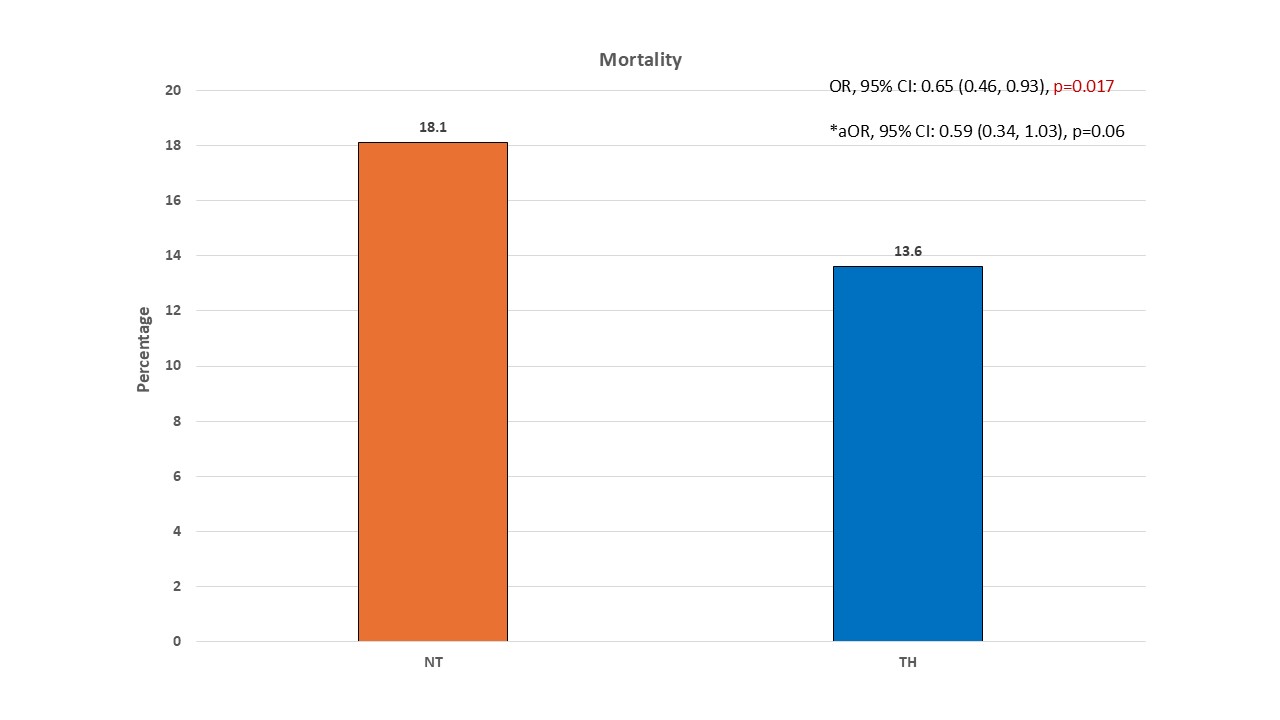
Background: Therapeutic Hypothermia (TH) in infants ≥35 weeks gestational age (GA) with moderate/severe hypoxic-ischemic encephalopathy (HIE) is associated with improved neurodevelopmental outcomes. A recent trial in preterm infants' 33-35 weeks GA with moderate to severe HIE found increased probability of harm with TH. Objective: To describe the association between TH and mortality in preterm infants 33-35 weeks GA with HIE treated with normothermia (NT) or TH. Design/Methods: The Children's Hospitals Neonatal Consortium (CHNC) database was queried to identify preterm infants with HIE or central nervous system depression between 2010-2025. Infants were stratified by receipt of TH. Severity of encephalopathy was graded as mild, moderate, severe, or unknown. Clinical, demographic and short-term outcomes data on mortality, neuroimaging and discharge with a feeding tube were collected. Data were analyzed using Chi-square and Fisher's exact tests. Generalized linear models with random intercept for center (clusters) were adjusted for encephalopathy severity. Results: Of 1,048 infants, 618 (58.9%) received TH and 430 (41.1%) received NT. The majority of infants offered TH were outborn, were of higher GA and birth weight, and had moderate or severe encephalopathy (Table 1). Mortality occurred in 162/1048 (15.5%) ; 84/618 (13.6%) in TH vs. 78/430 (18.1%) in NT group (unadjusted OR, 95% CI: 0.65 (0.46, 0.93), p=0.017). In adjusted analyses, the lower mortality in the TH group did not persist (aOR, 95% CI: 0.59 (0.34, 1.03), p=0.06) (Figure 1/Table 2). In infants with moderate/severe encephalopathy (n=613), unadjusted mortality was lower in the TH group (79/494,16.0%) compared to NT group (36/119, 30.3%) (OR, 95% CI: 0.42 (0.26, 0.67), p< 0.001) and at 35 weeks GA (OR, 95% CI: 0.27 (0.12, 0.65), p=0.003). However, the reduction in mortality was not observed after adjustment (aOR, 95% CI: 0.59 (0.34, 1.03), p=0.064) or at 35 weeks GA (aOR, 95% CI: 0.61 (0.21, 1.81), p=0.374. 110/691 (15.9%) infants were discharged on tube feeds, with no significant difference between groups (aOR: 0.93 (0.44-1.94), p=0.84). Among survivors with brain MRI (n=510), infants in TH group had more than fourfold higher odds of a normal MRI (aOR, 95% CI: 4.14 (2.06, 8.29), p< 0.001), and among those with moderate or severe encephalopathy (aOR, 95% CI: 3.92 (1.7, 9.03), p=0.001) (Table 2).
Conclusion(s): In infants treated with TH, mortality tended to be lower while survivors had four-fold higher odds of normal MRI. The benefit of TH in this population should be interpreted cautiously.
Table 1: Selected Clinical, Demographic and Birth Data (* shows missing data)
Figure 1: Mortality in preterm Infants 33-35 weeks gestational age treated with NT or TH. Unadjusted and adjusted Odds ratio, 95% CI are shown. *aOR: adjusted Odds ratio
Table 2: Mortality, neuroimaging and tube feedings at discharge in preterm infants 33-35 weeks treated with NT and TH

.jpg "Rakesh Rao, MD (he/him/his) photo")
.jpg)
.jpg)
