52 - Oral Feeding Outcomes at Hospital Discharge in Infants with Grade 2–3 Bronchopulmonary Dysplasia: A Single-Institution Review
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2049.52
Xiaolong Zhang, Chengdu women's and children's central hospital, Chengdu, Sichuan, China (People's Republic); Julia Welc, Children's Hospital of Philadelphia, Philadelphia, PA, United States; Kathleen A.. Nilan, Children's Hospital of Philadelphia, Chalfont, PA, United States; Huayan Zhang, Children's Hospital of Philadelphia-University of Pennsylvania, Philadelphia, PA, United States
Inpatient Clinical Supervisor Children's Hospital of Philadelphia Philadelphia, Pennsylvania, United States
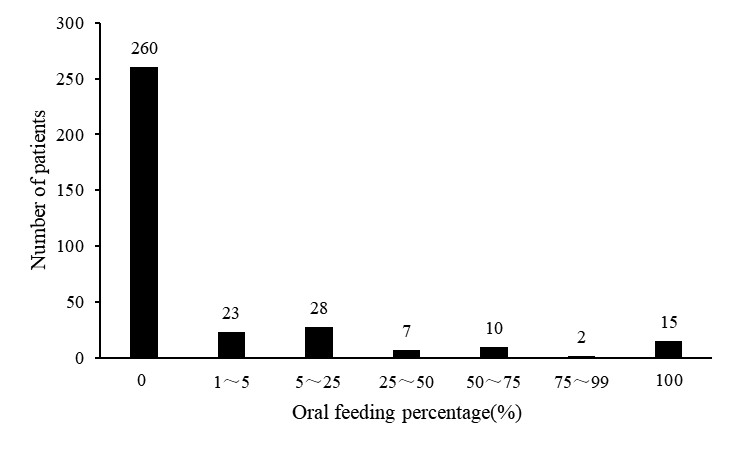
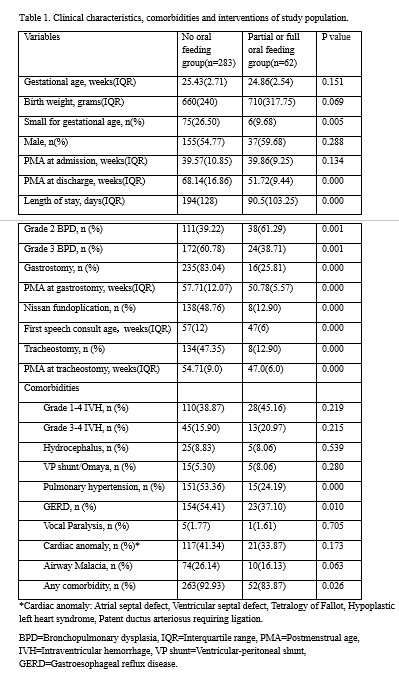
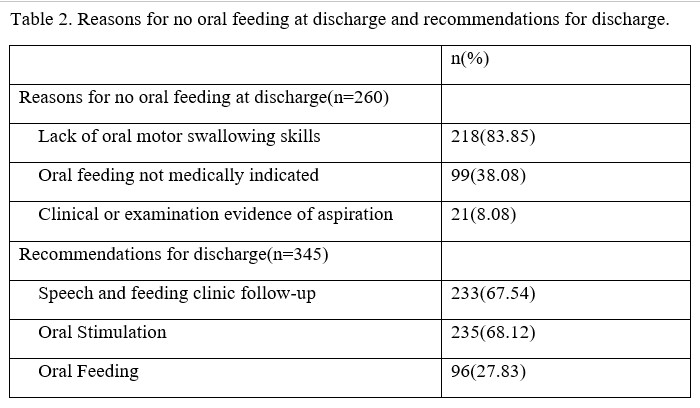
Background: Advances in neonatal care have increased the survival of premature infants with bronchopulmonary dysplasia (BPD). However, achieving safe and efficient oral feeding remains a significant challenge in these infants, contributing to delayed oral feeding milestones and prolonged hospitalizations. Since many hospitals do not have the ability of thoroughly evaluate the oral feeding safety in infants, this problem may be under recognized and under reported. Objective: To describe oral feeding status at time of hospital discharge and identify clinical factors associated with feeding outcomes in infants with grade 2-3 BPD. Design/Methods: This is a retrospective study of infants followed by the Newborn and Infant Chronic Lung Disease Program at the Children's Hospital of Philadelphia between January 2015 and June 2023. Infants with grade 2-3 BPD as classified using Jensen criteria were included. Patients who were deceased prior to discharge or had chromosomal abnormalities were excluded. All infants were formally evaluated by speech therapists for oral feeding abilities. Data collected included demographics, comorbidities, respiratory and surgical interventions, feeding status at discharge (none, partial, or full oral feeding), results of feeding skill evaluations. Statistical analyses used t-tests, Mann-Whitney U, and chi-square tests with significance set at p< 0.05. Results: Among 345 infants reviewed, 283 (82%) were discharged without oral feeding, 47 (13.6%) had partial oral feeding, and 15 (4.4%) achieved full oral feeding. Infants without oral feeding had longer hospital stays, greater PMA at discharge, and were more likely to have grade 3 BPD. They more frequently required gastrostomy, fundoplication, or tracheostomy and had higher prevalence of pulmonary hypertension and gastroesophageal reflux disease. Primary reasons for lack of oral feeding included poor oral motor coordination, aspiration risk, and medical instability. Most were referred for outpatient feeding follow-up and home oral stimulation.
Conclusion(s): Infants with grade 2-3 BPD face substantial barriers to achieving oral feeding by discharge. This may be related to disease severity and associated comorbidities. Early multidisciplinary assessment, targeted oral motor intervention, and caregiver education are essential to optimize feeding outcomes. Prospective studies are needed to evaluate structured oral stimulation programs and safe initiation of feeding in infants on increased respiratory support.
Figure 1. Percentage of oral feeding at discharge
Table 1. Clinical characteristics, comorbidities and interventions
Table 2. Reasons for no oral feeding at discharge and recommendations for discharge