537 - Early dexamethasone administration in croup: secondary analysis of the Better Assessment and Response to Croup in Kids (BARCK) Collaborative
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2522.537
Amy M. DeLaroche, Children's Hospital of Michigan, Detroit, MI, United States; Gabrielle Z. Hester, Essentia Health, Duluth, MN, United States; Amanda J. Nickel, Children's Hospitals and Clinics of Minnesota, Minneapolis, MN, United States; Kelly R.. Bergmann, Children's Minnesota, Minneapolis, MN, United States; Irina Topoz, University of Colorado School of Medicine, Aurora, CO, United States; Brittany Jennings, American Academy of Pediatrics, Itasca, IL, United States; Kendall Arslanian, American Academy of Pediatrics, Chicago, IL, United States; Bolanle T. Akinsola, Emory University School of Medicine, Atlanta, GA, United States; Beth A. Condley, University of Oklahoma Fran & Earl Ziegler College of Nursing, Norman, OK, United States; Daniela Hochreiter, Yale School of Medicine, New Haven, CT, United States; Adolfo Molina, University of Alabama School of Medicine, Birmingham, AL, United States; Amanda Nedved, Children's Mercy, Lenexa, KS, United States; Lisa Schroeder, Children's Mercy Hospitals and Clinics, Olathe, KS, United States; Ryan K. Sewell, Children's Nebraska, Omaha, NE, United States; Randi Trope, Stony Brook Children's Hospital, Stony Brook, NY, United States; Vivian Lee, Children's Hospital Los Angeles, Los Angeles, CA, United States; Amy Tyler, Nationwide Children's Hospital, Columbus, OH, United States
Faculty Children's Hospital of Michigan Detroit, Michigan, United States
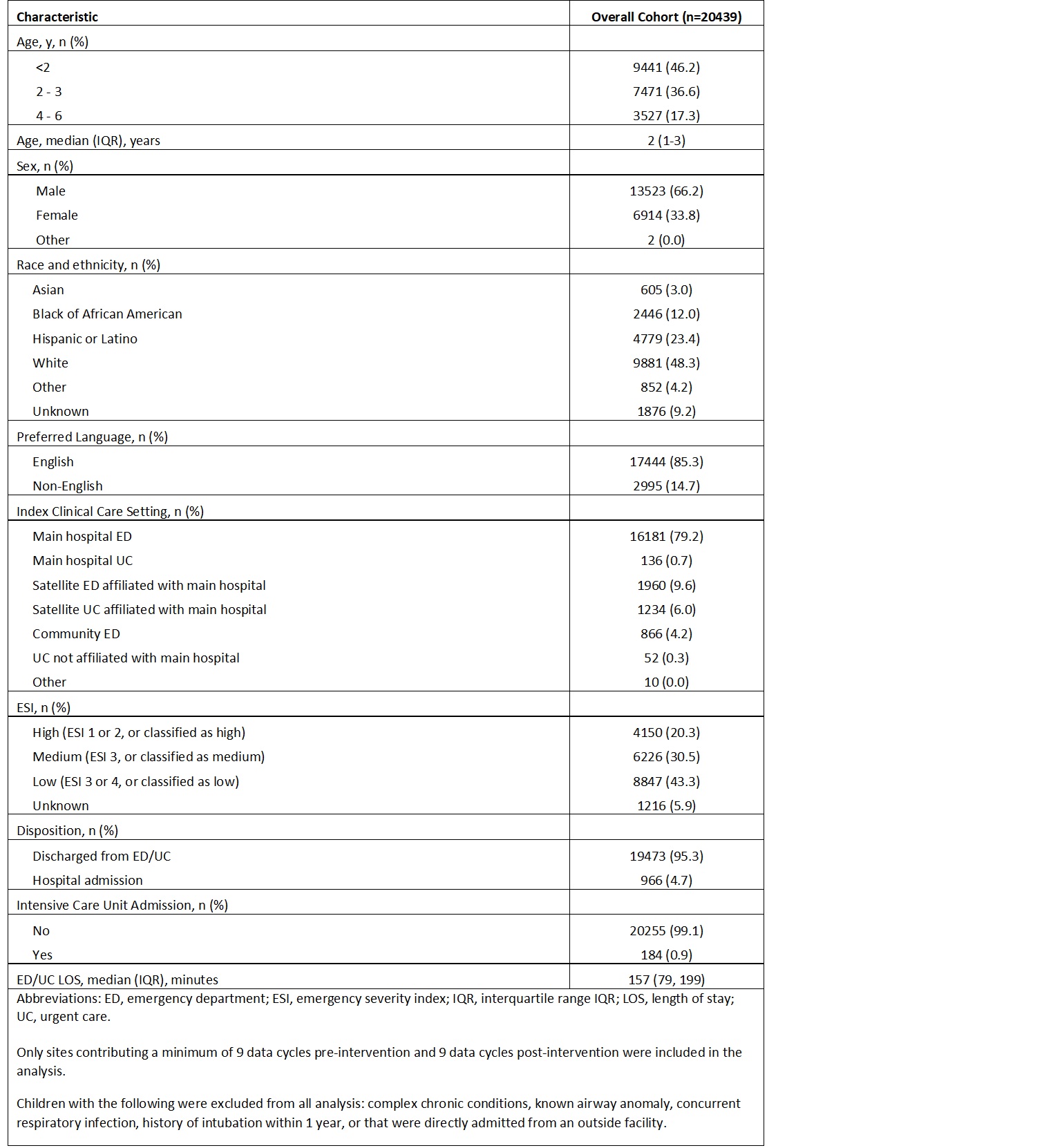
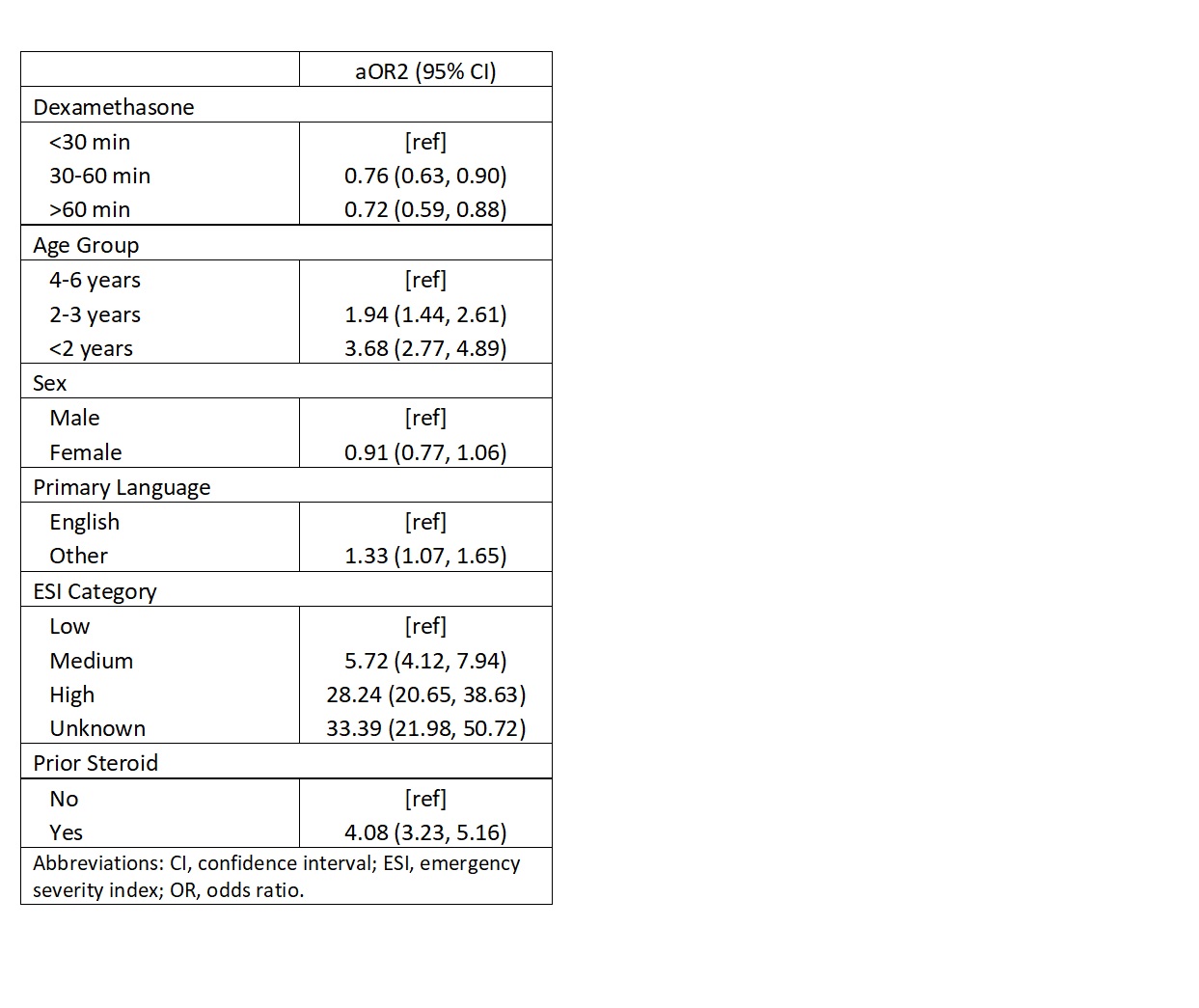
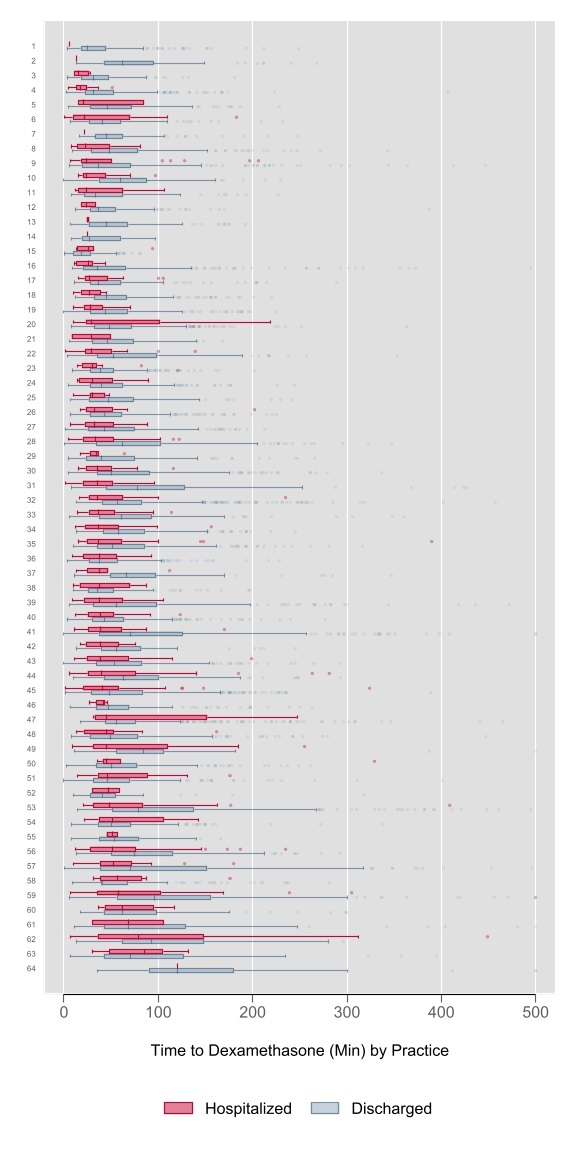
Background: Evidence supports a single dose of oral dexamethasone for all patients with croup. Timely administration is recommended, but it is unclear whether variation exists in the timing of dexamethasone administration, and whether early administration impacts clinical outcomes such as hospitalization. Objective: To (1) describe variation in the timing of dexamethasone administration, and (2) determine whether early dexamethasone administration is associated with hospitalization. Design/Methods: We conducted a planned secondary analysis of data from the multi-institutional Better Assessment & Responses to Croup in Kids (BARCK) quality improvement (QI) initiative. We included children 6 months to ≤ 6 years with a primary diagnosis of croup, treated with dexamethasone in a participating emergency department (ED) or urgent care (UC) between Jun 16, 2024 and Aug 15, 2025 (baseline Jun 16, 2024 to Jan 15, 2025; implementation Jan 16, 2025 to Aug 15, 2025). The primary outcome was hospitalization. Children were categorized based on the timing of dexamethasone ( < 30, 30-60, or >60 minutes) and a mixed-effects logistic regression model for hospitalization was performed, including a random intercept for site. The model was adjusted for age group, sex, primary language, severity of presentation, and receipt of a corticosteroid before ED/UC presentation. Intra-class correlation coefficients (ICC) were used to describe the percent variability attributed to a specific factor. Results: Across 65 participating sites, a total of 20,439 encounters were included and 966 (4%) were hospitalized (Table 1). The median time to dexamethasone administration differed significantly between discharged (50 minutes; IQR 31, 81) and hospitalized (38 minutes; IQR 24, 66; p< 0.0001) patients, with substantial variability in the median time to dexamethasone administration across sites (Figure 1). In multivariate logistic regression analysis, patients who received dexamethasone 30 - 60 minutes (aOR 0.76, 95% CI 0.63, 0.90) or >60 minutes after arrival (aOR 0.72, 95% CI 0.59, 0.88) had a lower odds of hospitalization compared to those who received dexamethasone < 30 minutes after arrival (Table 2). QI cycle and practice setting combined accounted for 20% [ICC 0.20 (0.14, 0.27)] of the variability in hospitalization.
Conclusion(s): The timing of dexamethasone administration varied across practice settings, indicating opportunities for QI. While we found croup patients were more likely to be hospitalized following early dexamethasone administration, there may be confounding factors not accounted for in our model as this is unlikely to be causative.
Table 1. Demographic and clinical characteristics of patients receiving dexamethasone upon urgent care or emergency department presentation
Table 2. Adjusted odds ratio
Figure 1. Variation in the timing of dexamethasone administration by practice site