528 - Reducing Racial Disparities in Asthma Care: Initiating Inhaled Corticosteroids for Pediatric Patients with Poorly Controlled Asthma in the Emergency Department
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2513.528
Angela Amaniampong, Childrens Hospital of Philadelphia, philadelphia, PA, United States; Bianca Nfonoyim Bernhard, Childrens Hospital of Philadelphia, Cherry hill, NJ, United States; Steven M. Rich, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Michael Bouvette, Childrens Hospital of Philadelphia, Palmyra, IN, United States; Emem Kierian, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Alicia Brandemarte, Childrens Hospital of Philadelphia, Philadelphia, PA, United States; Joseph J. Zorc, Childrens Hospital of Philadelphia, Wynnewood, PA, United States
Pediatric Emergency Medicine Fellow Childrens Hospital of Philadelphia Philadelphia, Pennsylvania, United States
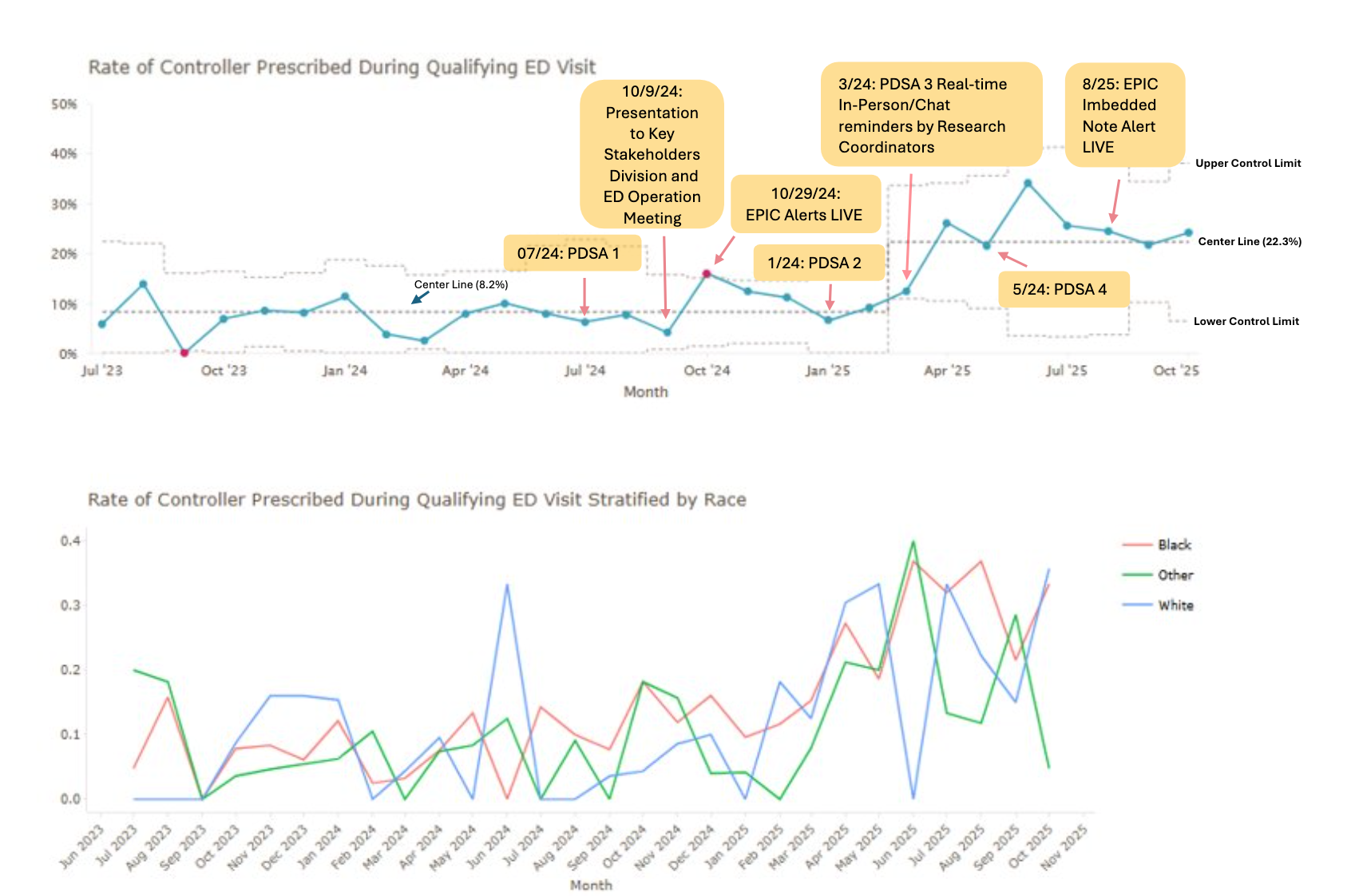
Background: Global Initiative for Asthma guidelines recommend initiating inhaled corticosteroid (ICS) medications at ED discharge for patients with uncontrolled asthma. However, national and local data reveal persistently low prescribing rates and limited evidence of effective implementation strategies with persistent disparities across race and ethnicities. To address this gap, we conducted a quality improvement (QI) project to develop and evaluate a novel approach for initiating ICS in the pediatric ED to improve outcomes and reduce disparities in asthma care. Objective: Increase the initiation rate of ICS for patients with uncontrolled asthma being discharged from the Pediatric Emergency Department from 6.3% to 25% by April 2025 across patients of all race and ethnicity groups. Design/Methods: We convened a multidisciplinary group to review current practices, develop driver diagrams, and test interventions through Plan-Do-Study-Act (PDSA) cycles as detailed in Table 1. Using institutional guidelines, we defined uncontrolled asthma as not currently prescribed an ICS and receiving 2 oral steroid courses within the past 6 months for children < 5 years of age or within the past 12 months for children ≥5 years of age. Key Drivers: Surveys of ED providers identified key drivers, including provider buy-in regarding the importance of prescribing ICS and decision support to guide prescription. Interventions in PDSA cycle one focused on education around prescribing guidelines. Interventions 2 and 3 added EHR alerts and provider feedback. Data was automated with manual chart review. The rate of ICS initiation (outcome measure) was monitored using a P chart. ED Length of Stay (LOS) was our balancing measure. Results: Analysis demonstrated non-random special cause variation consistent with sustained improvement attributable to our interventions. ICS initiation increased from a baseline of 6.3% to 15.9% after the first month and 34% by the eighth month with the center line increasing from 8.2% to 22.3%. Analysis stratified by race revealed that implementations remained equitable across racial groups. Average ED LOS increased by 2.2 minutes overall, while patients prescribed a controller after implementation had a mean LOS 21.5 minutes longer than those without prescription.
Conclusion(s): This QI project increased prescription of ICS at ED discharge through iterative PDSA cycles without substantially increasing ED LOS, and demonstrated equitable impact with no evidence of widening racial disparities in prescribing. Future efforts will investigate the impact of ICS initiation on outcomes such as ED revisit rates and PCP follow up
Timeline of strategies and interventions conducted and planned to improve the inhaled corticosteroid prescribing rate in the pediatric emergency department
Rate of Controller Prescribed During Qualified ED Visit

 Credit")
 photo")
.png)