Session: Infectious Diseases 2: Antimicrobial and Diagnostic Stewardship
406 - Patterns and Predictors of Non-First-Line Antibiotic Prescribing for Acute Respiratory Infections in the Pediatric Urgent Care
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2394.406
Nicita Anand, University of Missouri-Kansas City School of Medicine, Olivette, MO, United States; Amanda Nedved, Children's Mercy, Lenexa, KS, United States; Jennifer McKinsey, Children's Mercy Kansas City, Overland Park, KS, United States; Brian R. Lee, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Rana E. El Feghaly, Children's Mercy Kansas City, UMKC, Kansas City, MO, United States
Medical Student University of Missouri-Kansas City School of Medicine Olivette, Missouri, United States
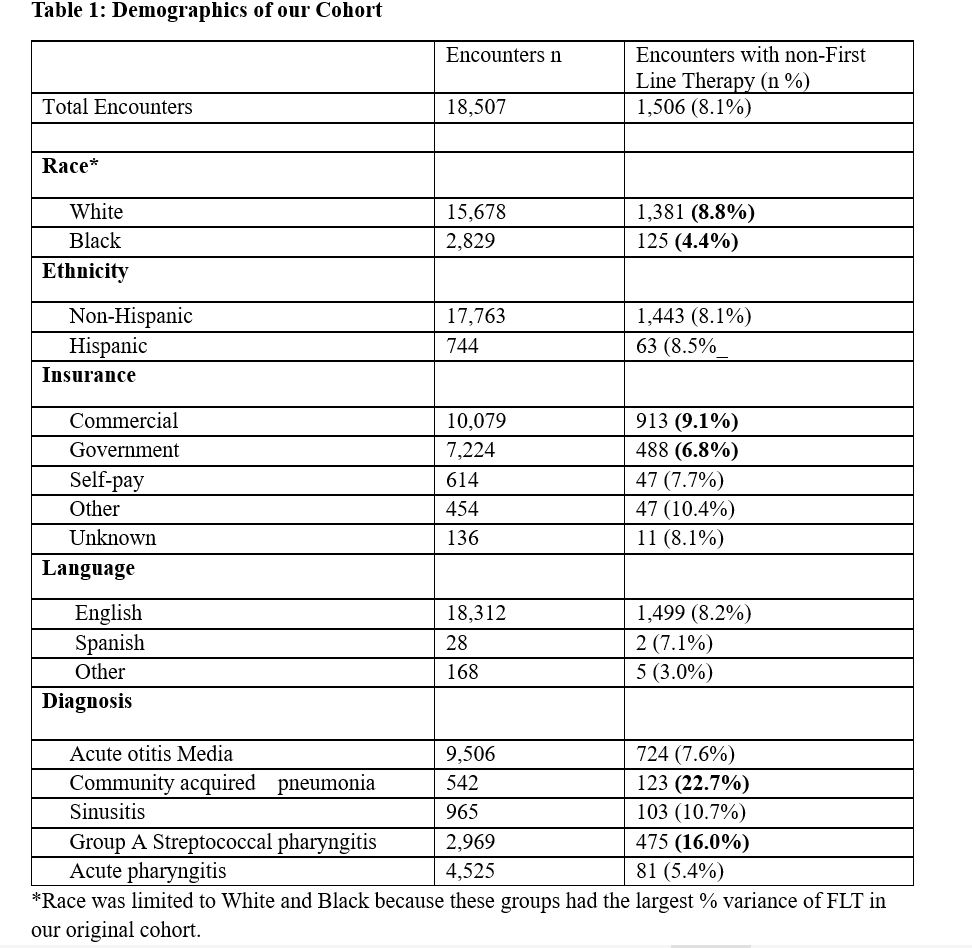
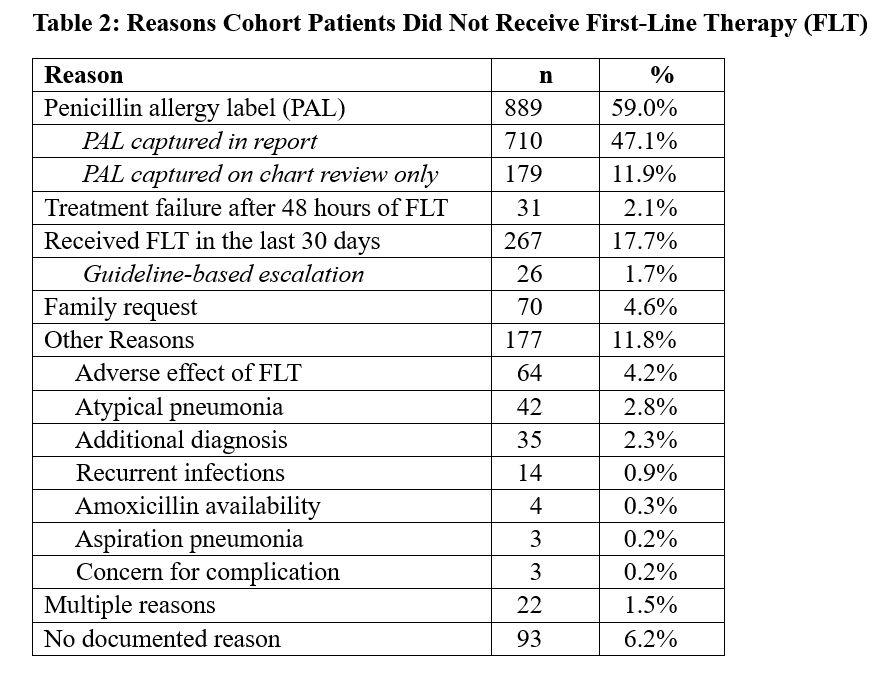
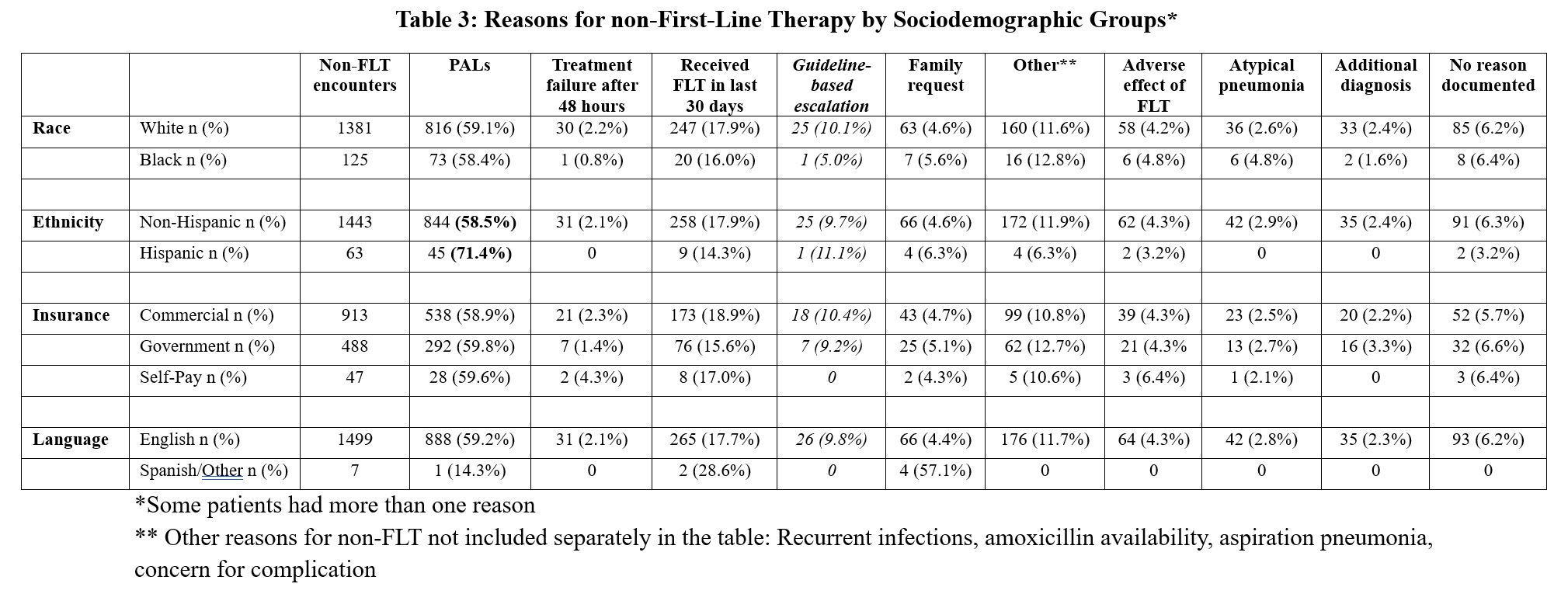
Background: Acute respiratory infections (ARIs) are the most common indication for antibiotic prescribing in pediatric ambulatory settings. Differences in first-line therapy (FLT) for ARIs have been observed across patient socioeconomic and demographic groups. Objective: To examine patient and system-level factors associated with non-FLT prescribing for ARIs in pediatric urgent care centers (PUCs). Design/Methods: We conducted a retrospective chart review of ARI encounters at three PUCs within a Midwestern academic center seen between April 2022 and March 2023. We defined FLT using national guidelines. We reviewed all encounters of acute otitis media (AOM), pneumonia, sinusitis, and pharyngitis in which patients were not prescribed FLT. We categorized encounters by diagnosis, demographic variables, and documented reasons for non-FLT use which included penicillin allergy labels (PALs), antibiotic use within the last 30 days, family request, treatment failure, other, and unknown reasons. Demographic variables included race (limited to White and Black), ethnicity, insurance type, and language. Results: Of 18,507 ARI encounters, 1,506 (8.1%) received non-FLT prescriptions for ARIs. Rates of non-FLT were higher in White compared to Black patients (8.8% vs 4.4%) and in patients with commercial versus government insurance (9.1% vs 6.8%) (Table 1). The most frequent reason for non-FLT prescribing was a PAL (n=889, 59.0%), followed by prior receipt of antibiotic within 30 days (n=267, 17.7%). Notably, only 26 (9.7%) of these escalations were consistent with guideline recommendations. Family request (4.6%), adverse effects (4.2%), and treatment failure (2.1%) were less common reasons for non-FLT prescribing (Table 2). Hispanic patients were more likely to receive non-FLT prescriptions due to PALs than non-Hispanic patients (71.4% vs. 58.5%). We did not find other significant variances among sociodemographic groups (Table 3).
Conclusion(s): In this cohort, over half of non-FLT prescriptions were attributed to PALs, with the next frequent reason related to escalation in therapy. However, most escalations to non-FLT were not consistent with guideline recommendations. Reasons for non-FLT had overall similar rates regardless of race, language or insurance; but Hispanic patients had higher rates of PAL-driven non-FLT compared to non-Hispanic patients. Implementing penicillin allergy de-labeling initiatives and improving clinician education on appropriate antibiotic escalation may improve FLT prescribing and promote more equitable antibiotic prescribing in PUC settings.
Table 1: Demographics of our Cohort
Table 2: Reasons Cohort Patients Did Not Receive First-Line Therapy (FLT)
Table 3: Reasons for non-First-Line Therapy by Sociodemographic Groups*