515 - Small Kidneys with a Big Impact: Investigating Kidney Size and Chronic Kidney Disease Vulnerability in Ugandan Children
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2500.515
Sarah Rogal, Joseph M. Sanzari Children's Hospital Hackensack University Medical Center, Fair Lawn, NJ, United States; Michael D. Lintner-Rivera, Riley Hospital for Children at Indiana University Health, Indianapolis, IN, United States; Michael Goings, Indiana University School of Medicine, Indianapolis, IN, United States; Anthony Batte, Makerere University, Kampala, Kampala, Uganda; Denver Brown, Children's National Health System, Washington, DC, United States; Stuart L.. Goldstein, CincinnatiChildrens, Cincinnati, OH, United States; Andrea Conroy, Indiana University School of Medicine, Indianapolis, IN, United States
Pediatric Nephrology Attending Joseph M. Sanzari Children's Hospital Hackensack University Medical Center Fair Lawn, New Jersey, United States
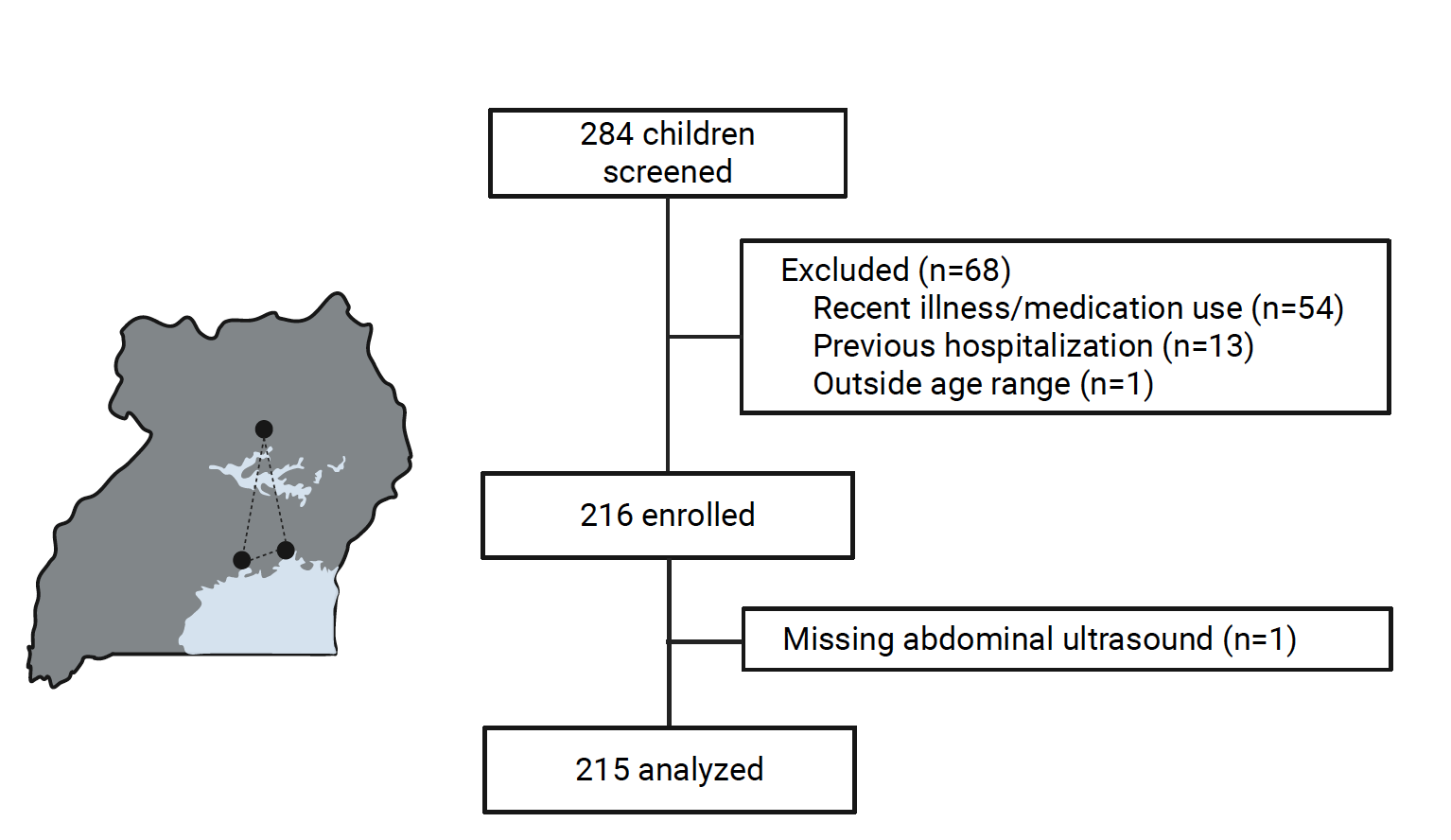
Background: Nephrogenesis completes at around 36 weeks of gestation. You are born with the maximal amount of nephrons that are unable to regenerate. Risk factors that impact nephron endowment, such as prematurity and low birthweight (LBW) are associated with hypertension, proteinuria, and chronic kidney disease (CKD) later in life. Kidney size is a surrogate marker for nephron endowment. Most studies assessing nephron endowment have been conducted in high-resource settings and normative data from low resource settings are lacking. Objective: To measure kidney size and assess for risk factors that contribute to small kidney size in Ugandan children. Design/Methods: We used data from 215 Ugandan children, 3 months to 16 years of age who were enrolled in the multi-site prospective study of malaria and CKD. Kidney size was obtained using ultrasounds performed from September 2023 through May 2025. Children were excluded if hospitalized or ill within the previous 4 weeks. General Additive Models for Location Scale and Shape were fit to compare kidney size to standard norms. Small kidney size was defined as bilateral small kidneys less than 2.5th percentile for height. Chi-square and t-tests investigated associations between perinatal, social, and environmental variables and small kidneys. Univariate and multivariate logistic regression was performed to look at risk factors for small kidney outcomes. Results: Average age of the cohort was 5.5 years old and 42.8% were female. Compared to European norms, Ugandan children had smaller kidneys independent of age, height, and body surface area (BSA). In comparing Ugandan children with normal and small kidney size, there was no significant difference with regard to glomerular filtration rate (GFR), hypertension, and proteinuria. LBW, maternal malaria during pregnancy, and maternal HIV status were not significantly associated with small kidney size. Low maternal mid-upper arm circumference (19-23 cm), a measure of maternal undernutrition, was independently associated with small kidney size (OR 2.97, CI 1.3-4.6) when controlling for child's age, BSA, recruitment site, maternal malaria, and LBW.
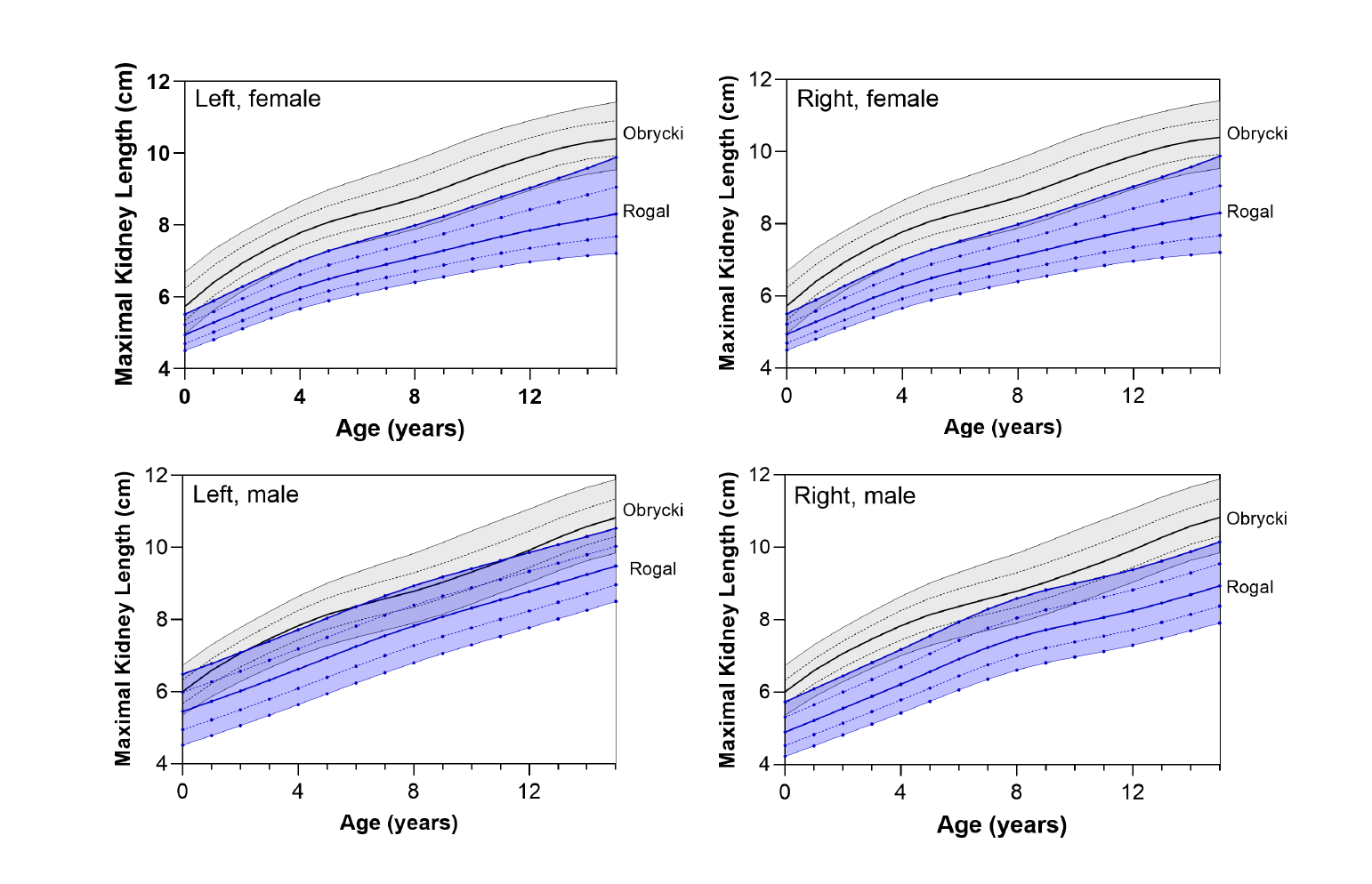
Conclusion(s): Ugandan children had universally smaller kidneys when compared to a healthy European cohort. Maternal under nutrition appears to be independently associated with small kidney size. Health and nutrition during pregnancy remain key factors in overall child health and may impact long-term kidney health and risk of CKD. Long term follow up is important to determine if a child's kidney size has clinical significance in CKD sequelae as they approach adulthood.
Recruitment of Children in Uganda
Growth Curves of Maximal Kidney Length Versus Age Compared to European Cohort

 photo")