321 - Landscape of Medicaid Managed Care Add-ons for Pediatric Asthma
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2310.321
Anna Chorniy, Icahn School of Medicine at Mount Sinai, New York, NY, United States; Anton Chorniy, Northwestern University, Chicago, IL, United States; Matthew M. Davis, Nemours Children's Health, Wilmington, DE, United States
Assistant Professor Icahn School of Medicine at Mount Sinai New York, New York, United States
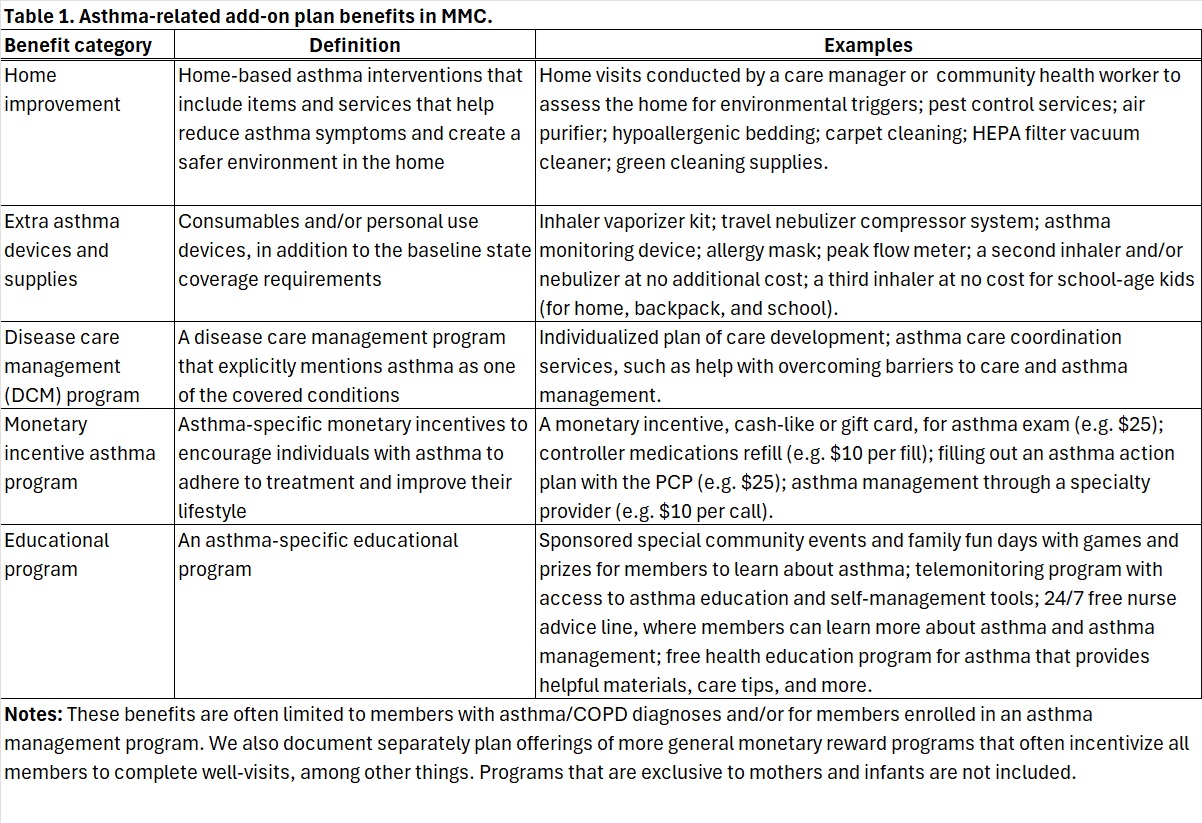
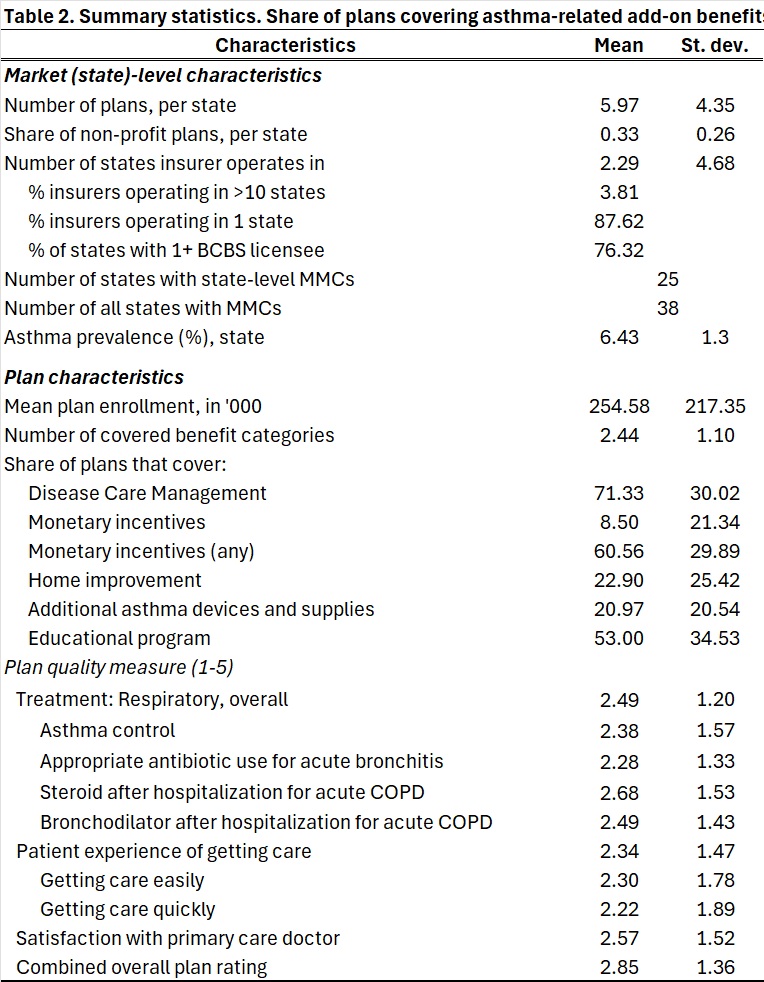
Background: Asthma affects over five million U.S. children, causing impaired quality of life, disability, and preventable death. It imposes major economic costs on families and the healthcare system. There are nearly 650,000 asthma-related child emergency department (ED) visits annually and asthma is the third leading cause of hospitalization among children. Despite therapeutic advances, ED visits and mortality rates have changed little over the past decade. Medicaid covers more than 35 million children under age 19. With 75% now enrolled in Medicaid Managed Care (MMC), plan design is central to care quality. While prior studies compare MMC with fee-for-service, less is known about the discretionary "value-added" or "add-on" benefits MMC plans provide beyond required services. These offerings may influence utilization and outcomes, yet systematic evidence on their availability and scope is limited. Objective: To describe the national landscape of asthma-related MMC add-on benefits for children, assess variation in benefit type and quality, and examine associations with insurer, market, and geographic factors. Design/Methods: We integrated data from 2023-2024 on plan characteristics, quality performance, and state context. Data were collected from all states with at least one comprehensive MMC organization, excluding those with region-specific contracts. Asthma-related add-ons were identified from publicly available plan materials accessible to enrollees before plan selection and linked to NCQA's Healthcare Effectiveness Data and Information Set (HEDIS), including Asthma Medication Ratio and satisfaction scores. Additional Medicaid.gov data verified parent organization, reimbursement model, and enrollment. Descriptive regression analyses related add-on benefits to insurer, market, and area characteristics. Results: States averaged six MMC plans (range: 3-9). One-third were non-profit, with an average of 255,000 enrollees per plan. Among plans offering asthma-related add-ons, 71% included disease care management, 61% offered incentives, 53% provided education, 23% covered home improvements, and 21% supplied extra asthma devices. Plans covered an average of 2.4 of six benefit categories. Plan quality ratings averaged 2.5 for respiratory care and 2.9 overall.
Conclusion(s): Asthma-related MMC add-ons vary widely across states and plans. Most include management and education programs, but few address environmental or material supports that reduce triggers. Greater transparency and integration of add-on benefit information into state plan assignment and oversight could enhance quality and equity in pediatric asthma care.