535 - Clinical Predictors of Chest Radiography Use in Pediatric Asthma Exacerbations
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2520.535
Alexander H. Hogan, Connecticut Children's, Hartford, CT, United States; Alek C. Jorge, Connecticut Children's Medical Center, Berlin, CT, United States; Annina Beus, Connecticut Children's Medical Center, Hartford, CT, United States; Richelle deMayo, University of Connecticut School of Medicine, Westport, CT, United States; Assaf Landschaft, Boston Children's Hospital, Bergisch Gladbach, Nordrhein-Westfalen, Germany; Ilana Waynik, Connecticut Children's Medical Center, West Hartford, CT, United States; Amir Kimia, Connecticut Children's Medical Center, Boston, MA, United States; Noah Sobel, University of Connecticut School of Medicine, Farmington, CT, United States
Associate Professor of Pediatrics Connecticut Children's Hartford, Connecticut, United States
Background: Chest radiography (CXR) during pediatric acute asthma exacerbations is discouraged due to high false-positive rates, as atelectasis is often misinterpreted as bacterial infection. Despite this, ordering rates remain above 30%. Objective: To identify (A) the reasoning documented by providers for ordering CXRs and (B) the clinical risk factors associated with CXR use in children presenting with respiratory symptoms and either a history of asthma or a clinical presentation consistent with asthma. Design/Methods: This retrospective cross-sectional study included children aged 2 to 18 years who presented to the Connecticut Children's Emergency Department between July and December 2024. Eligible patients had respiratory symptoms with either a history of asthma or a clinical presentation consistent with asthma, as identified from the clinical narrative. We selected this approach, rather than relying on ICD-10 discharge codes, to capture patients with a clinical presentation of asthma, rather than only those assigned an asthma diagnosis at discharge.
We trained a natural language processing (NLP) classifier and reviewed its output using a sensitivity threshold of 95%. Data identified by the NLP model were manually reviewed by trained clinicians. Demographic and clinical data, as well as provider-documented reasoning for obtaining a CXR, were extracted.
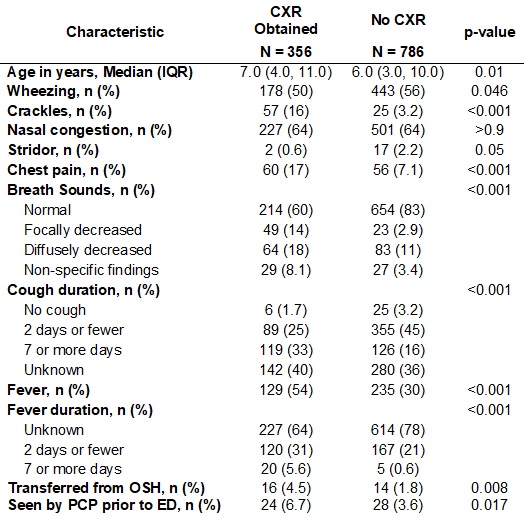
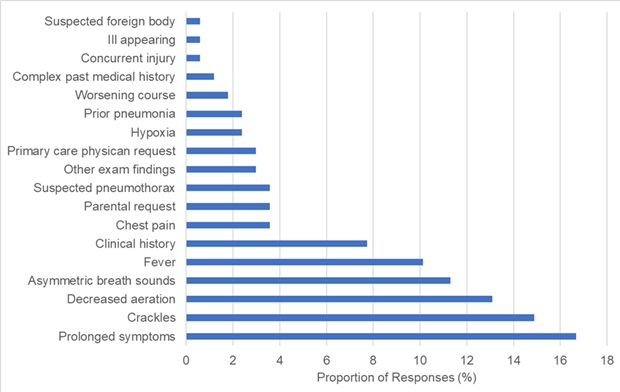
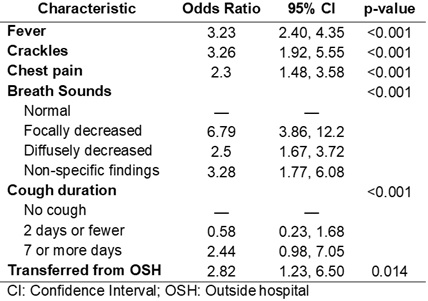
A multivariable logistic regression model was developed to identify factors independently associated with CXR utilization. The model was fit using maximum likelihood estimation with a binomial family and logit link function. Results are reported as adjusted odds ratios with 95% confidence intervals, and statistical significance was assessed at p< 0.05. Results: Among 1,143 emergency department encounters for respiratory conditions in children with asthma or treated for asthma, 356 received a chest X-ray (31%, Table 1). Provider reasoning for CXR ordering was documented in 46% of cases. The most commonly cited reasons included prolonged symptoms, crackles on exam, and decreased aeration (Figure 1). In multivariable analysis, the strongest predictors of CXR use were focal lung findings, the presence of crackles, and a history of fever (Table 2).
Conclusion(s): In children presenting to the emergency department with respiratory symptoms and possible asthma exacerbation, clinical exam findings were the strongest predictors of CXR use. Efforts to reduce unnecessary CXR utilization must address clinician perceptions of these exam findings, particularly given the known low diagnostic yield of imaging in these scenarios.
Clinical characteristics of those who received a CXR
CXR Justification per Clinical Documentation (If Present)
Multivariable Regression of Risk Factors for Obtaining CXR