183 - Feasibility, Recruitment, and Retention of a Multi-State, Longitudinal Study of Parents' Newborn Screening Experiences
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2176.183
Kelly Christensen, Children's National Hospital, Gaithersburg, MD, United States; Anne Atkins, Children’s National Hospital, Madison, WI, United States; Brianne Zielinski, BrownWinick Law Firm, Waukee, IA, United States; Thevaa Chandereng, Children's National Health System, Washington, DC, United States; Christen Crews, Virginia Department of Health, Midlothian, VA, United States; Lindsay Cooper, Johns Hopkins University School of Medicine, Phoenix, MD, United States; Tia Tyson, Children's National Health System, Hyattsville, MD, United States; Knute Carter, University of Iowa College of Public Health, Iowa City, IA, United States; Lisa Opipari-Arrigan, Children's National Health System, Cohasset, MA, United States; Tara Lavelle, Tufts Medical Center, Boston, MA, United States; Beth A. Tarini, Co-Director, Silver Spring, MD, United States
Data Manager Children's National Hospital Gaithersburg, Maryland, United States
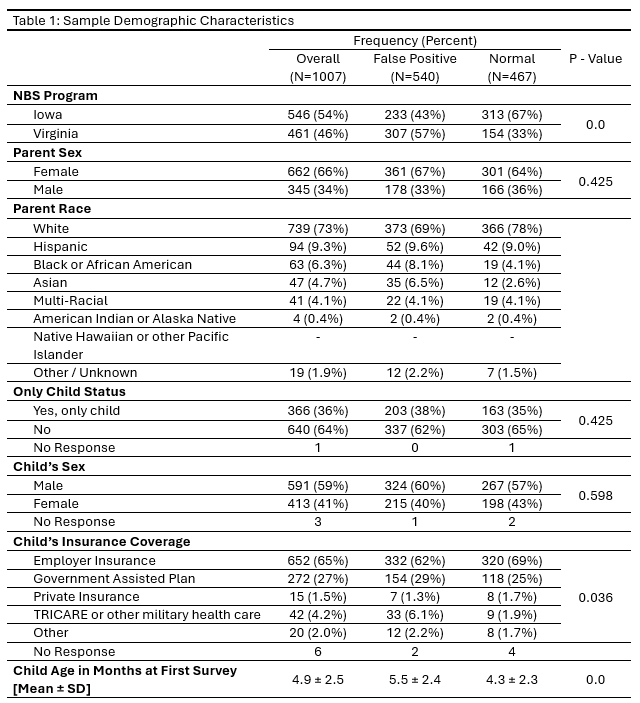
Background: Most studies of parents' experiences with newborn screening (NBS) are small, single-site, or cross-sectional focusing on true positive diagnoses. To date, there have been no multi-site, prospective, longitudinal studies that follow parents after they have received NBS results. Such research is essential to advancing high-quality, evidence-based strategies that optimize NBS result deliver for the 3.5 million families screened annually in the US. Objective: To collaborate with NBS programs to recruit parents for a longitudinal, population-based study examining parents' experiences after receiving a false positive (FP) or normal (NL) NBS result. Design/Methods: In partnership with the Iowa and Virginia NBS programs, we conducted recruitment from Summer 2020 through March 2023. Parents who received FP or NL NBS results were initially contacted by mail and followed up by phone to obtain verbal consent. An initial survey assessed demographics and NBS experience. Longitudinal surveys at child age 6, 12, 18, and 24 months assessed psychological outcomes. Descriptive and comparative analyses examined recruitment, demographic, and participation patterns by recruitment site and cohort. Results: A total of 1,083 parents (718 families; 15% overall recruitment) were enrolled in 3 years. Both parents were enrolled for 52% of families. Total enrollment was similar across sites, but VA had a higher proportion of FP parents (79% vs 43%). Recruitment method and child age varied by site, with IA parents enrolled earlier than VA parents (mean child age at first survey IA: 3.2±1.5 months, VA: 7.0±1.5 months, p-value: 0.0). 93% of parents enrolled completed the first survey, with 1,007 included in analyses. Retention across all five surveys was 64%. Demographically our parents were female (66%), White (73%), and married (79%). Race and ethnicity in our study sample was representative of IA and VA state demographics.
Conclusion(s): In the first multi-site, longitudinal study of parent experiences following NBS results, our findings demonstrate successful recruitment and retention of parents, including fathers and those receiving NL NBS results. Partnerships with public health NBS programs are vital; they require reliable support from the study team and their institution. This study provides a roadmap for scaling population-based NBS outcomes research across diverse jurisdictions.