280 - Time-To-Care for Children with Suboptimal Child Passenger Safety Practices in Fatal Crashes
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2270.280
Arthi S. Kozhumam, Northwestern University The Feinberg School of Medicine, Chicago, IL, United States; Mech Frazier, Northwestern University, Chicago, IL, United States; MIchelle Macy, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States
MD-PhD Candidate Northwestern University The Feinberg School of Medicine Chicago, Illinois, United States
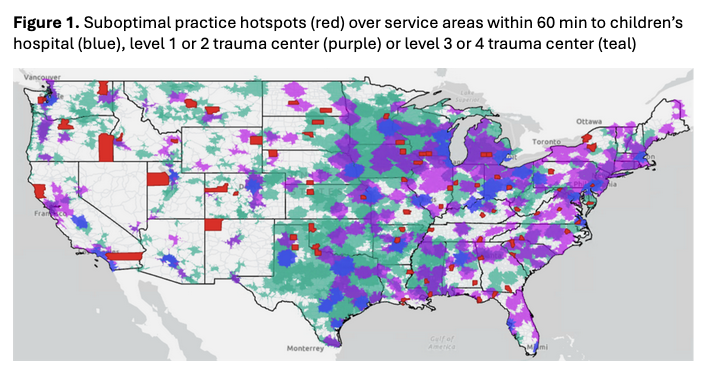
Background: After a motor vehicle crash (MVC), treatment within the "golden hour" improves injury outcomes. Children with suboptimal child occupant protection (Table 1) are at risk of being more severely injured in an MVC than those who are correctly using an age-appropriate restraint. Little is known about EMS transport times for children in MVCs, relative to their occupant protection practices, or their access to a trauma center within 60 minutes. Objective: 1. Compare time-to-care for children involved in a crash in the Fatality Analysis Reporting System (FARS) who had appropriate vs suboptimal child occupant protection. 2. Identify overlap between counties that are suboptimal protection hotspots in FARS and crash locations > 60 minutes to a trauma center by level. Design/Methods: We categorized child occupant protection as appropriate or suboptimal based on the American Academy of Pediatrics Child Passenger Safety Policy Statement (Table 1) and identified 75 US county hotspots for suboptimal protection based on FARS data, 2011-2021. Crash coordinates and injury severity (0-4, no injury to fatal injury) were also extracted from FARS. We extracted coordinates of trauma centers (levels 1-4) and children's hospitals from the American Hospital Association. ArcGIS Network Analyst Toolbox was used to identify MVCs >60 min to trauma center care across levels via road network analysis. Descriptive, t-test and chi square statistics were calculated using RStudio. Results: FARS included 38,037 child occupants < 13 with known CRS, seating position, and MVC coordinates; 26,582 (70%) had suboptimal occupant protection. 10% of children with suboptimal protection were outside 60 min to care compared with 8% of those appropriately restrained. Children with suboptimal protection had slightly longer time-to-care than children appropriately restrained (median 21 min, IQR 12-38 vs 20 min, IQR 11-35, p< 0.005). 43 of 75 (57.3%) suboptimal protection county hotspots included areas >60 min from a trauma center or children's hospital (Figure 1). Children with suboptimal protection, particularly those restrained in the front seat, experienced reduced trauma center access and higher injury severity than those appropriately restrained (Table 2).
Conclusion(s): Children involved in an MVC in suboptimal protection hotspots face long time windows from crash to trauma center, the minimum time-to-care on top of ambulance transport. Additional prehospital support to areas that are outside of the golden hour for children in MVCs with a focus on those who are front seat passengers can prioritize resources for children at high risk of injury in an MVC.
Table 1. Suboptimal practice components used in analysis
Figure 1. Suboptimal practice hotspots (red) over service areas within 60 min to children's hospital (blue), level 1 or 2 trauma center (purple) or level 3 or 4 trauma center (teal)
Table 2. Time to care and injury severity for children with appropriate vs suboptimal (overall, and by component) practices across trauma center level and injury severity

 photo")
.png)
.png)
