478 - Distance from Transplant Center and Associations with Pediatric Kidney Allograft Outcomes
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2466.478
Camille Chun, Children's Hospital Colorado, Denver, CO, United States; Joseph Chuita, Children's Hospital Colorado, Littleton, CO, United States; Margret Bock, University of Colorado School of Medicine, Aurora, CO, United States; Eric Benz, University of Colorado School of Medicine, Aurora, CO, United States
Pediatric Nephrology Fellow University of Colorado / Children's Hospital Colorado Denver, Colorado, United States
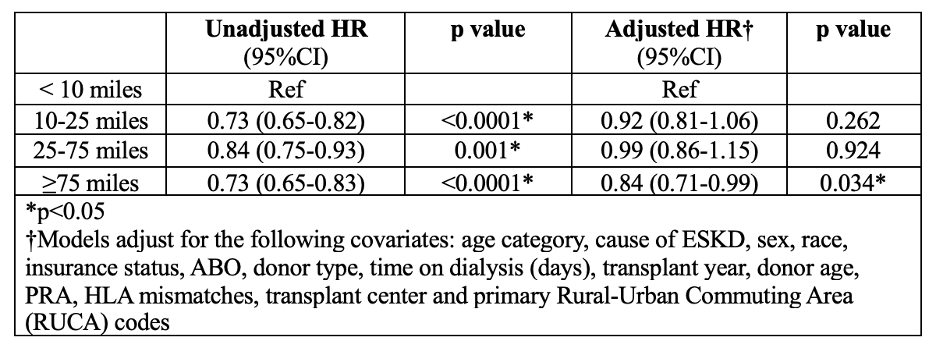
Background: Kidney transplantation (KT) offers improved survival compared with dialysis for children with End Stage Kidney Disease. Increased geographic distance from transplant center (TC) is associated with increased wait times for deceased donor KT and increased mortality while on the KT waitlist for children awaiting organ transplantation. Adult studies demonstrate recipient distance from TC is associated with increased mortality after KT. Impact of recipient distance to TC on post-transplant outcomes in pediatric KT is not well studied. Objective: Investigate whether increased geographic distance from TC is associated with allograft failure in pediatric KT recipients. Design/Methods: We performed a retrospective cohort study using the Scientific Registry of Transplant Recipients (SRTR) including incident pediatric ( < 21 years) KT recipients from 2003 - 2023. Inclusion criteria included availability of personal zip code information at time of transplant. Zip code data were used to estimate distance to TC by calculating nautical miles via geolocating a government address in each recipient zip code and mapping to TC address using ArcGIS software. Distance to TC was subdivided into quartiles for analysis. Associations with 1- and 5-year all-cause allograft failure were examined using multivariable cox proportional hazard models. Results: We included 16,764 patients in our study. There was no association with all-cause allograft failure at 1-year post transplant and distance from TC. Patients living ≥75 miles from their TC had decreased hazard of all-cause allograft failure at 5 years post-transplant (HR 0.84 [0.71-0.99]) when compared to those < 10 miles from the TC. There was no difference in allograft failure at 1- or 5-years post-transplant for patients living 10-25 miles or 25-75 miles from their TC when compared to those < 10 miles from TC.
Conclusion(s): Increased distance from TC, ≥75 nautical miles, is associated with decrease in 5-year all-cause allograft failure rates after pediatric KT (16% reduced risk of allograft failure at 5 years post-transplant). Further studies are needed to elucidate whether this finding is due to variations in pediatric clinical practices, whether unmeasured social determinants of health play a role in our findings, and whether opportunities to modify practices to improve outcomes for patients closer to their TC exist.
Association of distance to transplant center (nautical miles) and hazard of allograft failure at 5-years post-transplant

 photo")
.png)
