261 - Policy as prevention: A state-level framework for pediatric firearm injury prevention policy
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2251.261
Lauren Zaylskie, Indiana University School of Medicine, Terre Haute, IN, United States; Kelsey Gastineau, Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, TN, United States; Jason Yaun, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Katherine Purdham, University of Tennessee Health Science Center College of Medicine, Memphis, TN, United States; Hunter Butler, Monroe Carell Jr. Children's Hospital at Vanderbilt, Springfield, TN, United States
Medical Student Indiana University School of Medicine Terre Haute, Indiana, United States
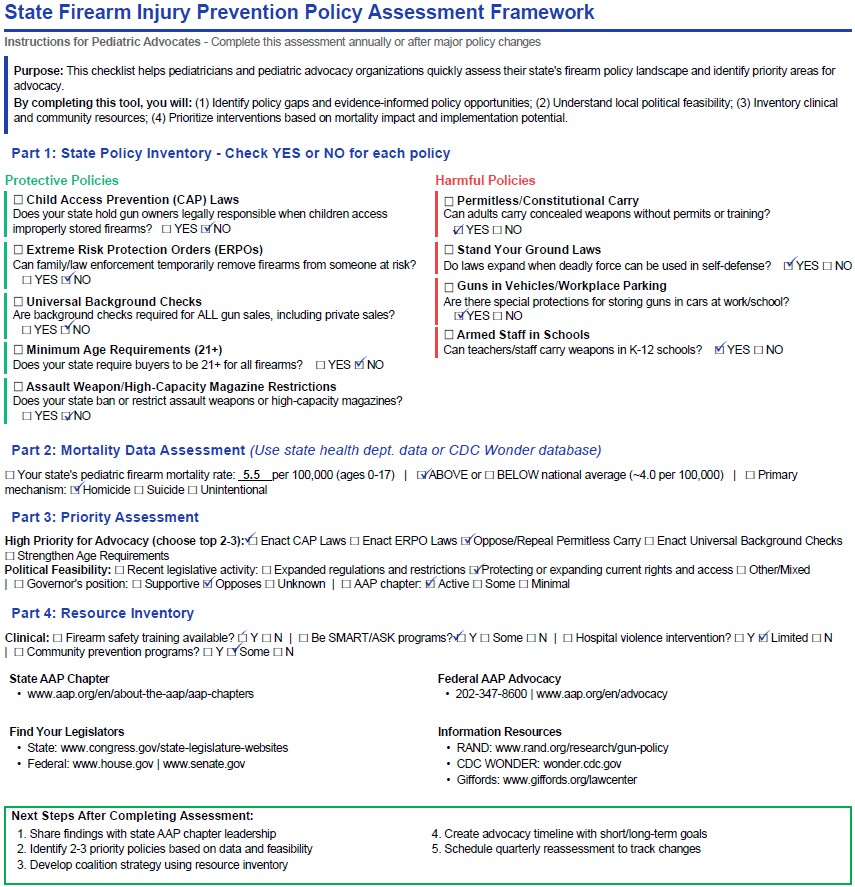
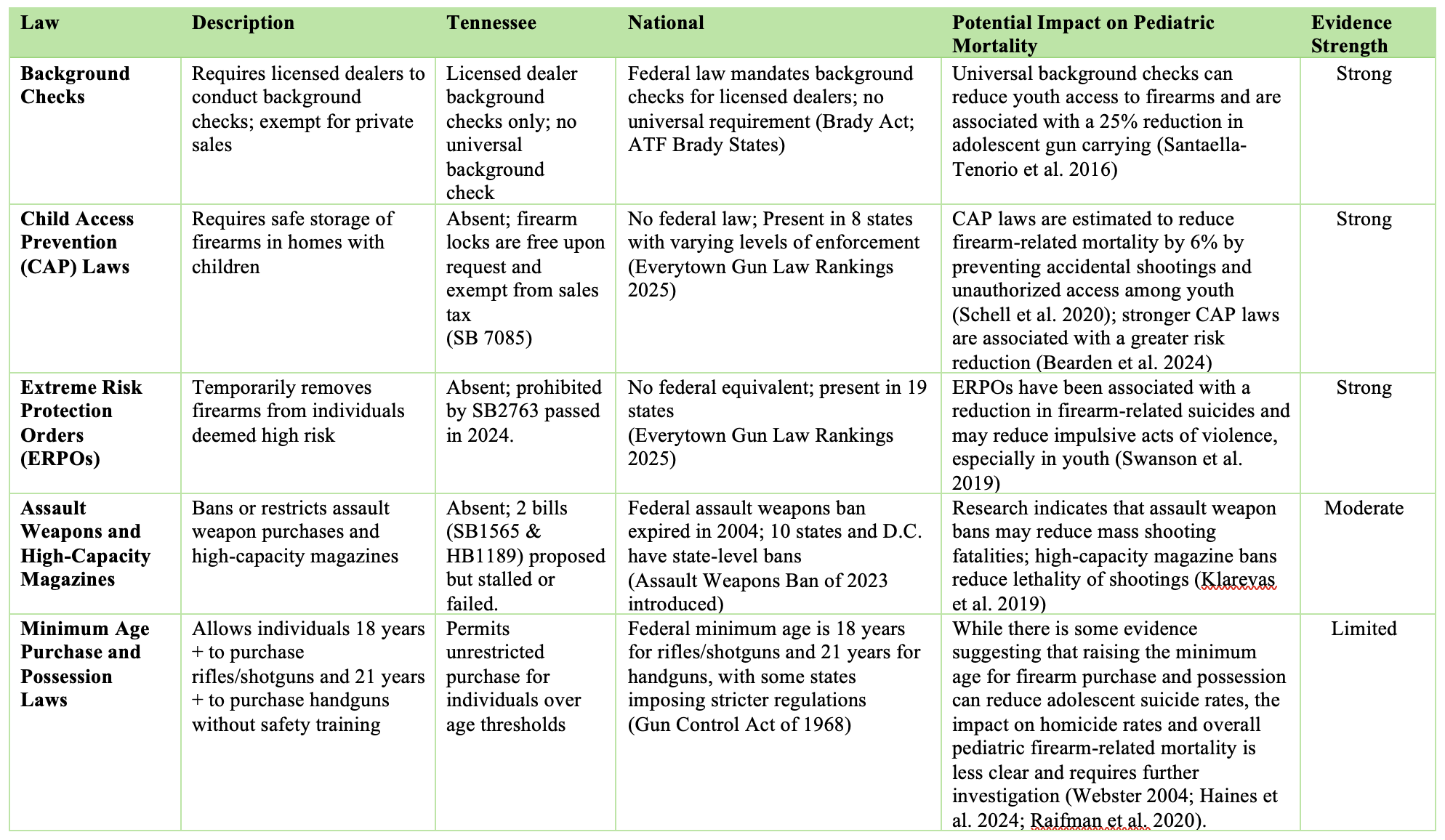
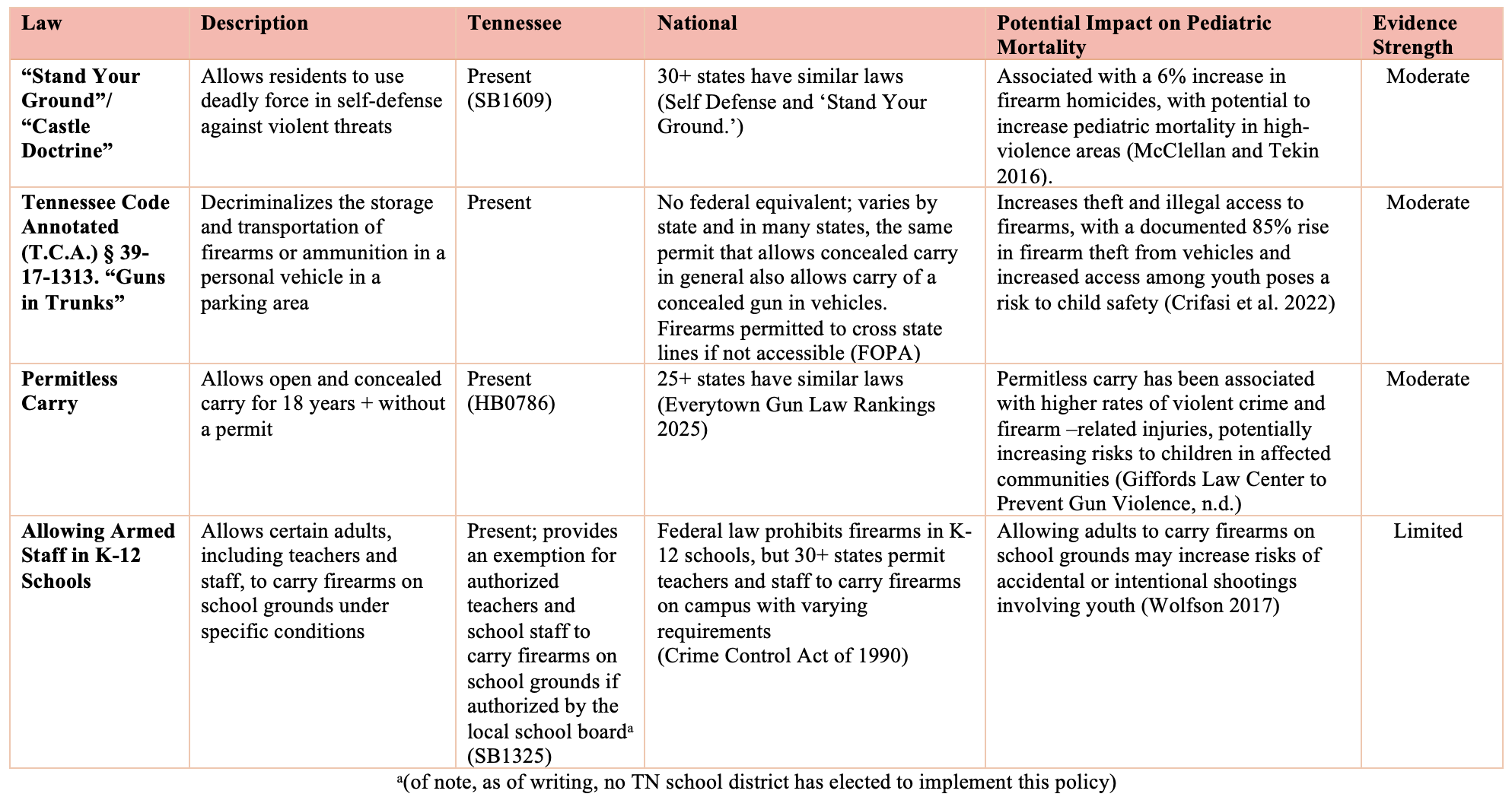
Background: Firearm injuries are the leading external cause of death for youth in Tennessee with a mortality rate 36% above the national average. Tennessee's firearm policy landscape is evolving yet has not been formally evaluated through the lens of pediatric morbidity, mortality, and advocacy. Objective: Review published evidence on firearm-related policies, identify policy gaps, create and apply a novel replicable assessment tool enabling pediatricians to use Tennessee as a guide for legislative advocacy efforts in their state. Design/Methods: We reviewed current Tennessee firearm legislation (2010-2024) and compared it to federal laws and policies in other states. We synthesized published evidence on firearm policy effectiveness using the RAND Gun Policy Research database and American Academy of Pediatrics guidelines. We applied the findings to Tennessee's policy landscape to identify gaps and develop prioritized, evidence-based recommendations. Finally, we created a structured assessment tool across four domains (Figure 1; with Tennessee as example). Results: Tennessee has minimal firearm regulations and several laws expanding firearm access, including permitless carry, "guns in trunks" provisions allowing firearm storage in vehicles, and authorization for armed school staff (Table 2). The state lacks Child Access Prevention (CAP) laws and Extreme Risk Protection Orders (ERPOs) which are associated with reduced pediatric firearm deaths and decreased firearm suicides, respectively (Table 1). Three priority recommendations for Tennessee emerged: (1) enact CAP laws to reduce unauthorized child access to firearms; (2) enact ERPO laws to enable temporary firearm removal for individuals at risk; and (3) expand clinical firearm safety counseling statewide. The resulting assessment tool provides a structured checklist for evaluating five protective policies (CAP laws, ERPOs, universal background checks, minimum age requirements, assault weapon restrictions) and four harmful policies (permitless carry, stand your ground laws, guns in vehicles, armed school staff), with guidance for linking state mortality data to advocacy priorities.
Conclusion(s): Tennessee's evolving firearm policy landscape includes limited evidence-based safety legislation and several laws expanding access. While this study did not directly assess causality, the alignment between policy gaps and elevated pediatric firearm mortality suggests areas for targeted advocacy. This framework provides a replicable model for pediatricians and advocacy organizations to assess state firearm policies, identify gaps, and develop evidence-based recommendations.
Figure 1: State Firearm Legislation Assessment Framework
Table 1: Comparison of Tennessee to National Firearm Legislation: Protective Policies
Table 2: Comparison of Tennessee to National Firearm Legislation: Harmful Policies

 photo")