50 - Bedside Flexible Endoscopic Evaluation of the Swallow (FEES) in the Neonatal Intensive Care Unit
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2047.50
Lotenna E. Kalu, Alberta Health Services, Medicine Hat, AB, Canada; Dianna Wang, University of Alberta Faculty of Medicine and Dentistry, Edmonton, AB, Canada; Eduard C. Eksteen, Children's Hospital, Edmonton, AB, Canada; Julia S.. Giesen, Alberta Health Services, Edmonton, AB, Canada; Brenda H. Law, University of Alberta, Edmonton, AB, Canada
Assistant Professor University of Alberta Edmonton, Alberta, Canada
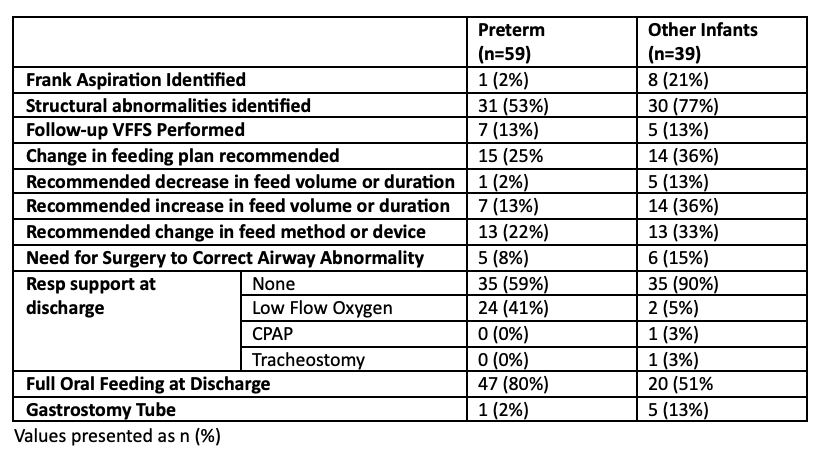
Background: Achieving oral feeding is an important neonatal milestone, impacted by lung disease, brain injury, genetic and airway conditions. New ultrathin fibreoptic bronchoscopes has made it possible for bedside Flexible Endoscopic Evaluation of the Swallow (FEES) to be done in the Neonatal Intensive Care Unit (NICU), allowing clinicians to evaluate swallowing in neonates while avoiding the radiation of Video Fluoroscopic Swallowing Exam (VFFS). There is limited data on bedside FEES in the NICU, particularly for infants on non-invasive respiratory support. Objective: To describe bedside FEES performed by a team of speech language pathologist, neonatologist, and otolaryngologist in a NICU. Design/Methods: This was a retrospective cohort of infants admitted to a Level 3 NICU who had documented bedside FEES from January 2022 to December 2024. Hospital charts were reviewed for demographics, respiratory support and feeding plan during FEES, indications for and results of FEES, adverse events during FEES, need for VFFS, and contribution of FEES findings to patient management, and outcomes. Results: There were two populations (n=98): 1) preterm infants and 2) infants with other primary diagnoses. Most (85%) had no adverse events during FEES. Only 7% needed the procedure terminated. For preterms (n=59), median birth gestation was 28+4 weeks (IQR 25+4-33+6), with a median birthweight of 1210g (IQR 795-1905g). 64% were on respiratory support (9 on LFNC, 24 on HFNC, 2 on CPAP, 3 on NIMV) during FEES. Most (81%) were receiving some oral feedings prior to FEES. Only one had aspiration noted. 52% had structural airway abnormalities identified. For other infants (n=39), median birth gestation was 38+2 weeks (IQR 37+2-39+4). The most common diagnoses were: hypoxic ischemic encephalopathy (9), genetic conditions (8), and congenital airway anomalies (7). 33% were on respiratory support (4 on LFNC, 8 on HFNC, 1 on CPAP) during FEES. 54% were receiving some oral feedings at prior to FEES. 8 infants (21%) infants had aspiration noted. 77% had structural airway anomalies identified. After FEES, only 12 patients had a follow-up VFFS. 30% had change in feeding plans. 11 infants had airway surgery post FEES, and 6 had gastrostomy tube inserted. At time of discharge, 24/59 (40%) preterms were on LFNC compared with 2/39 term infants. A lower proportion of preterm infants were discharged on any gavage feeds compared with infants with other diagnoses (17% vs 44%)
Conclusion(s): Bedside FEES performed by a multidisciplinary team is safe and helped guide feeding plans for a selected neonatal population.

 photo")
.png)