fellowship Chang Gung Memorial Hospital, Linkou branch Linkou, New Taipei, Taiwan (Republic of China)
Background: Thoracic fluid content (TFC), derived from thoracic electrical bioimpedance, inversely reflects intrathoracic fluid volume. Measured by Electrical Cardiometry (EC), a non-invasive cardiac output monitor applicable in preterm infants, TFC has been linked to pulmonary fluid overload in respiratory diseases. However, data on TFC in extremely preterm infants remain limited. Objective: This study aimed to establish reference ranges for TFC in hemodynamically stable extremely preterm infants during the early postnatal period and to examine its relationship with surfactant-treated respiratory distress syndrome (RDS) and significant patent ductus arteriosus (sPDA; ductal size ≥1.5 mm or left atrium-to-aortic root ratio >1.5). Design/Methods: This was a post-hoc analysis of a prospective cohort study that included multiple hemodynamic monitoring modalities in infants with a gestational age (GA) ≤28 weeks or birth weight (BW) ≤1000 g. Infants with major congenital anomalies, perinatal asphyxia, or those requiring post-resuscitation care were excluded. Continuous minute-to-minute EC monitoring was performed, complemented by daily targeted echocardiography during the first 72 hours of life. TFC values were averaged at 6-hour intervals from birth to 72 hours of age. Infants were classified as hemodynamically stable if they had no evidence of systemic fluid overload or depletion, did not require surfactant therapy, and had no sPDA. The generalized estimating equation (GEE) model was used to calculate the correlation between TFC and BW or PDA size, and to compare TFC between infants with and without RDS or sPDA. Results: A total of 30 extremely preterm infants (GA 27.1 ± 2.0 weeks, BW 830 ± 225 g) were enrolled. Among them, 10 infants met the criteria for hemodynamic stability, and reference TFC values were proposed (Figure 1). Significant positive correlations were observed in the GEE model between TFC and BW (β = 0.01, p = 0.001), and between TFC and ductal size after adjusting for BW (β = 12.5, p = 0.016). In addition, infants with both RDS and sPDA had significantly higher TFC values than those without (β = 8.19, p = 0.016) (Table 1).
Conclusion(s): Reference ranges for TFC in hemodynamically stable extremely preterm infants were established. The positive correlations suggest that TFC should be adjusted for weight in interindividual comparisons, and TFC associated with PDA shunting indicate increased pulmonary circulation. In infants with combined surfactant-treated RDS and sPDA, a synergistic effect on thoracic fluid accumulation was observed.
Reference values of TFC from day 1 to day 3 No significant time effect within timing points
Correlation of TFC with body weight, PDA diameter, and RDS combined with sPDA


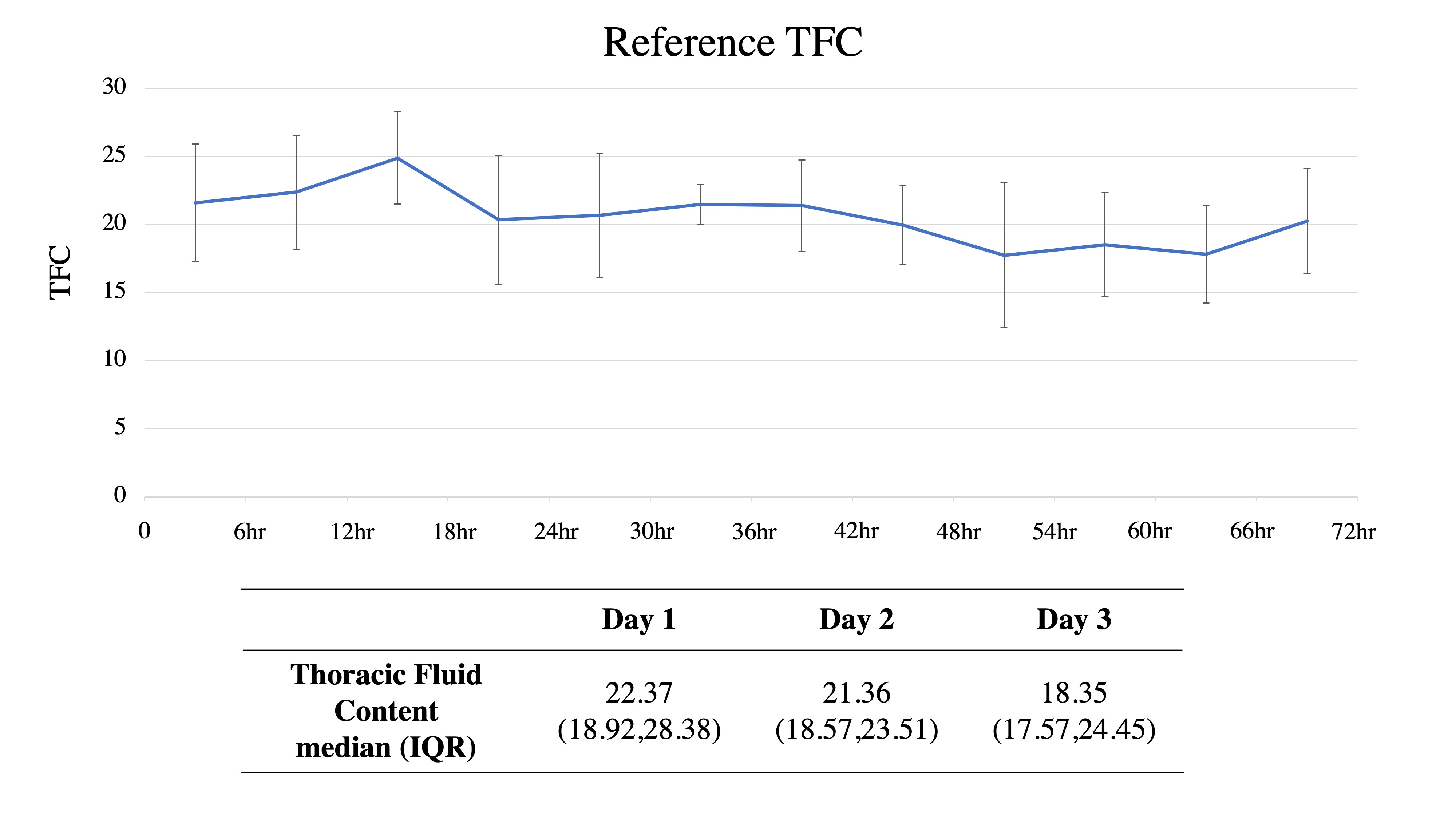 No significant time effect within timing points
No significant time effect within timing points .jpg)
