638 - Early Antibiotic Exposure and Brain Volumes in Preterm Infants: Insights from the REASON Trial
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2623.638
Diomel DE LA CRUZ, University of Florida, Gainesville, FL, United States; Arleena Rupnaraine, University of Florida College of Medicine, Gainesville, FL, United States; Nan Li, University of Florida, Gainesville, FL, United States; Kirill Luka, University of Florida, Gainesville, FL, United States; Nikolay Bliznyuk, University of Florida, Gainesville, FL, United States; Wei Shao, University of Florida College of Medicine, Gainesville, FL, United States; Josef Neu, University of Florida, Gainesville, FL, United States; Michael D.. Weiss, University of Florida, Gainesville, FL, United States
Neonatology Fellow University of Florida College of Medicine Gainesville, Florida, United States
Background: Empiric antibiotics are routinely used in symptomatic preterm infants to prevent early-onset sepsis, though most remain culture negative. This exposure overlaps with a critical period of gut and brain development, when microbial colonization and neural pathways interact through the gut-brain axis. The REASON trial showed that withholding antibiotics was safe, while sub-studies found reduced Veillonella and fecal GABA and tryptophan, suggesting altered microbial-brain signaling. This study examined whether early antibiotic exposure affected brain volume at term-equivalent age. Objective: To evaluate whether early empiric antibiotic exposure alters gut-brain signaling through microbiome and metabolomic changes that influence brain volume in preterm infants at term-equivalent age. Design/Methods: Infants ≤33 weeks' gestation without life-limiting anomalies were enrolled (n=98). Groups included: A, high-risk symptomatic infants treated with antibiotics (n=32); B, low-risk asymptomatic controls (n=11); and C, symptomatic infants randomized to antibiotics (C1, n=28) or none (C2, n=27). Because only two infants in Group B had MRI, they were excluded. C2 was further divided into C2B (bailed), infants randomized to no antibiotics but later treated at clinician discretion, and C2NB (not bailed), who remained antibiotic-free. C1 and C2B were combined as C3 to evaluate antibiotic exposure versus non-exposure (C2NB). Clinical data included demographics, maternal exposures, feeding type, and outcomes. Term-equivalent MRI (~36 weeks) used T2-weighted images analyzed with an AI-based 2.5D segmentation pipeline. See Diagram 1 and Table 1 Results: MRI data were available for 52 infants: Group A (n=17), C3 (C1+C2B, n=25), and C2NB (n=8). Groups were similar in gestational age, birth weight, and maternal exposures. Median length of stay was longest in Group A (85 days) and shortest in C2NB (67.5 days). Rates of bronchopulmonary dysplasia, retinopathy of prematurity, and other complications were comparable. MRI analysis showed no significant differences in total brain volume between groups or when comparing all antibiotic-exposed infants (C3) with unexposed (C2NB). See Diagram 2.
Conclusion(s): Early empiric antibiotic exposure was not associated with measurable differences in total brain volume at term-equivalent age. Global brain growth appeared preserved despite microbial and metabolomic alterations described in prior REASON analyses. Larger longitudinal studies integrating microbiome, metabolomic, and neuroimaging data are needed to define the long-term effects of early antibiotic exposure.
Diagram 2. Comparison of Brain Volumes amongst different subgroups Diagram2_ Comparison of Brain Volumes amongst Different subgroups.pdfDiagram 2. Group A included high-risk symptomatic preterm infants who received empiric antibiotics immediately after birth . Group C included symptomatic infants without infection risk who were randomized to antibiotics (C1) or no antibiotics (C2). Within Group C2, C2B (bailed) were infants initially randomized to no antibiotics but later treated at clinician discretion, while C2NB (not bailed) remained antibiotic-free. To evaluate the effect of antibiotic exposure, C1 and C2B were combined as C3 (antibiotic-exposed) and compared with C2NB (unexposed).


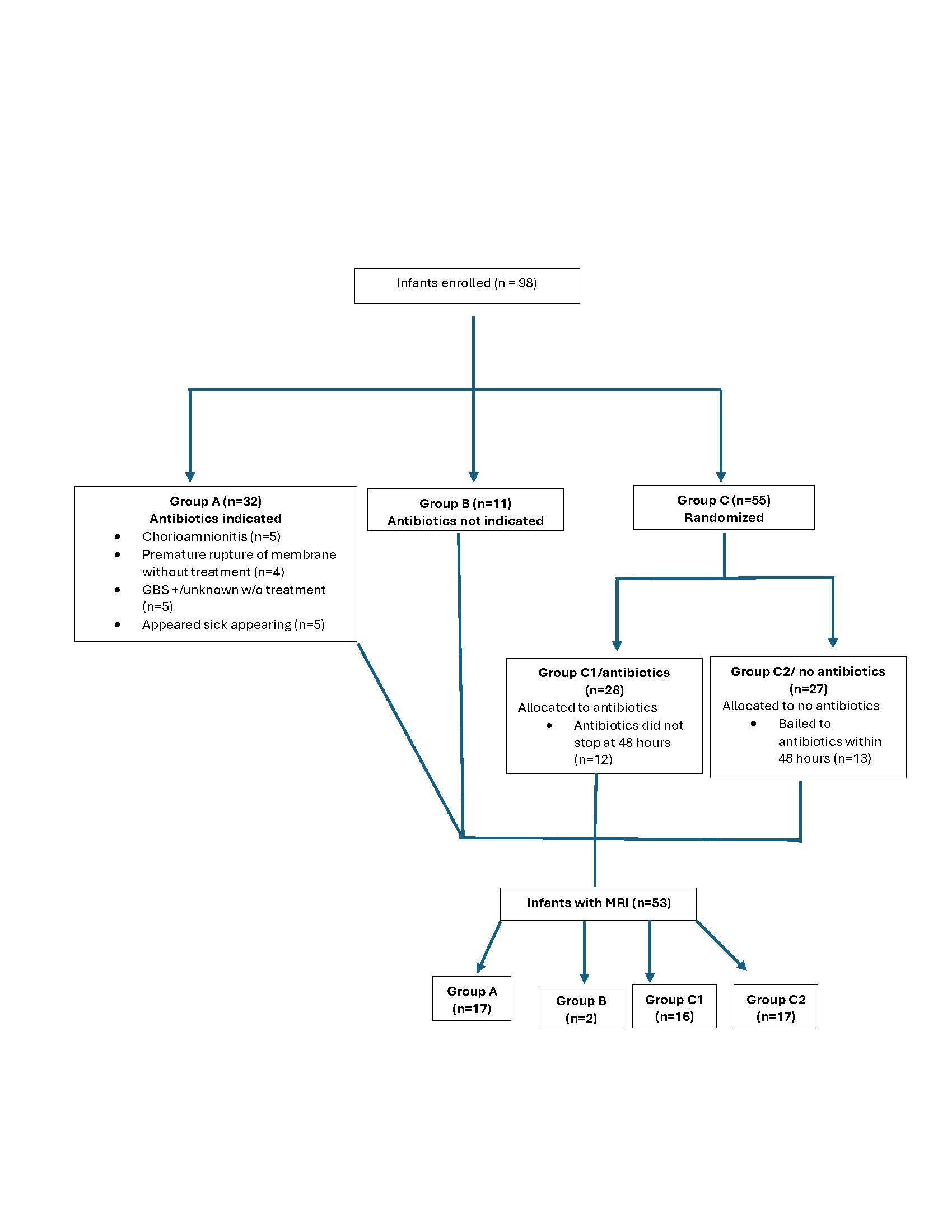 Diagram 1 . Subject Groupings
Diagram 1 . Subject Groupings