370 - A longitudinal assessment of participation and respiratory virus epidemiology in a multi-year school-based cohort of pre-kindergarten-12th grade students and school staff
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2359.370
Jennifer Goldman, Children's Mercy Kansas City, Kansas City, MO, United States; Rangaraj S. Selvarangan, Childrens Mercy Kansas City, -- Select one --, MO, United States; Brittney Fritschmann, Children's Mercy Hospital, Kansas City, MO, United States; Nibha sagar, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States; Dithi Banerjee, Children’s Mercy Hospital, Kansas City, MO, United States; Anjana Sasidharan, Childrens Mercy Hospital, Kansas City, MO, United States; Jennifer Schuster, Children's Mercy Kansas City, Kansas City, MO, United States; Brian R. Lee, Children's Mercy Hospitals and Clinics, Kansas City, MO, United States
Professor of Pediatrics Children's Mercy Kansas City Kansas City, Missouri, United States
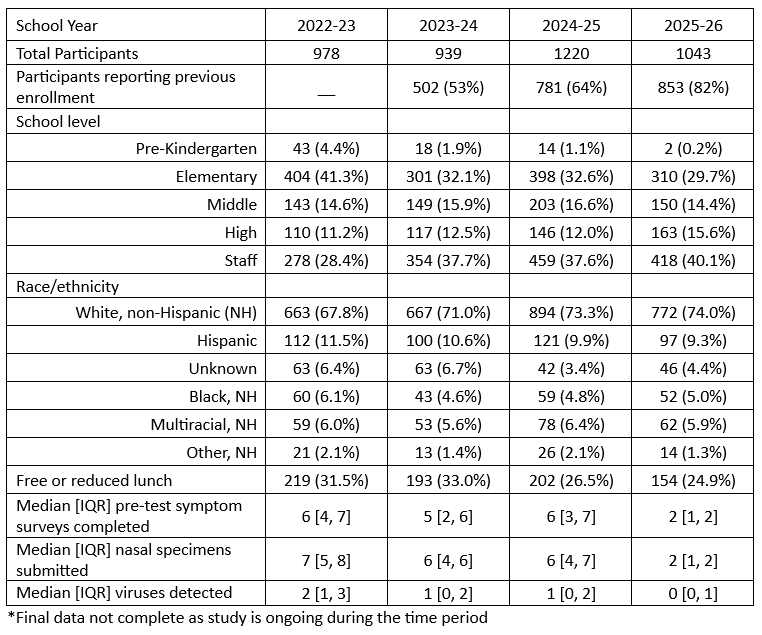
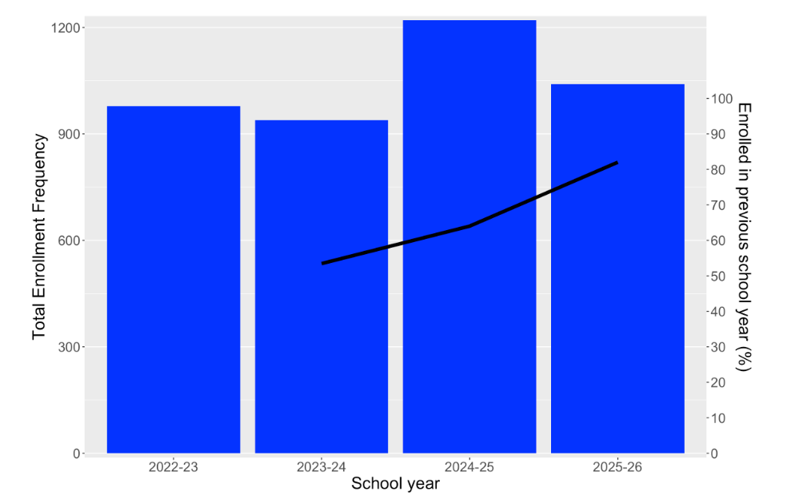
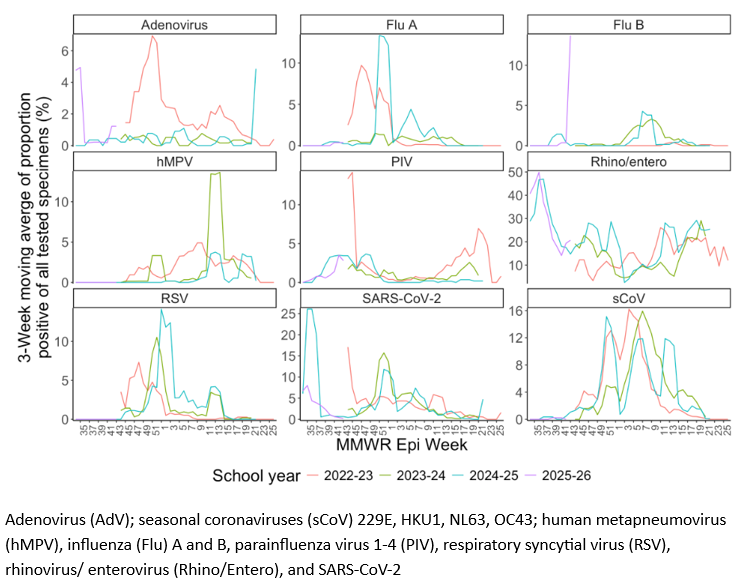
Background: Longitudinal respiratory viral surveillance can be challenging, particularly in the community setting. Schools provide a unique venue for longitudinal studies as most students and staff remain in a particular school district for several years. Objective: We set out to understand longitudinal participation and viral epidemiology in a respiratory surveillance program in prekindergarten - 12th grade during 4 consecutive school years. Design/Methods: Knowledge of Infectious Diseases in Schools (School KIDS) is a multi-year longitudinal respiratory virus surveillance program in a large, public kindergarten-12th grade school district in Kansas City, MO. For 4 consecutive school years (SY 2022-2026), students and staff voluntarily enroll annually to participate in monthly nasal specimen collection while at school (i.e., surveillance specimens) and symptomatic specimen collection when experiencing recent acute respiratory illness (ARI) symptoms (i.e., on-demand specimens). Prior to specimen collection, participants completed a text or email survey reporting the presence of ARI symptoms. Respiratory specimens were obtained using a self-administered nasal swab and tested by multiplex PCR. Analysis included participant enrollment by school year, completion of symptom surveys and respiratory testing, and virology trends. Results: Total enrollment of students and staff was 978 (SY22-23), 939 (SY23-24), 1220 (SY24-25), and 1043 (SY25-26) (Table 1). Participants reporting enrollment of prior study year increased over time 53% (SY23-24) vs. 82% (SY25-26), P < 0.001 (Figure 1) and 290/978 (30%) of SY22-23 participants participated in all 4 years of the study. Of those 290, the median number of viral detections was 5 [interquartile range (IQR) 3,7] and median number of surveys with ≥1 respiratory symptoms was 9 [IQR 5.75, 14]. On average, participants submitted a median of 6 symptom surveys and nasal specimens. Overall percent positivity for on-demand testing (47.4%) and surveillance testing (22.1%) remained steady during the study years, however, specific virus circulation varied by year (Figure 2). Unique peaks were observed in different years: adenovirus peaked in SY22-23 winter; human metapneumovirus peaked in early spring SY 23-24; and SARS-CoV-2 peaked at the beginning of SY24-25.
Conclusion(s): Retainment of School KIDS participants was high with >50% re-enrollment increasing annually suggesting strong program acceptance. Longitudinal studies in the school setting can generate valuable data to inform public health and estimate community rates of respiratory virus detection.
Table. Demographics of School KIDS participants
Figure 1. School KIDS enrollment over 4 school years and percentage of repeat enrollees
Figure 2. Percent positivity for viruses detected by school year