59 - Effects of Gestational Age and Maternal Morbidities on Infant Birth Weight in U.S. NICUs
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2056.59
Nicole Ferguson, Kennesaw State University, Kennesaw, GA, United States; Minaahil Cheema, Kennesaw State University, Cumming, GA, United States; Irene E. Olsen, Drexel University, Philadelphia, PA, United States; Reese H.. Clark, Duke University School of Medicine, Marietta, SC, United States; Jessica G. Woo, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, United States
Professor of Statistics Kennesaw State University Kennesaw, Georgia, United States
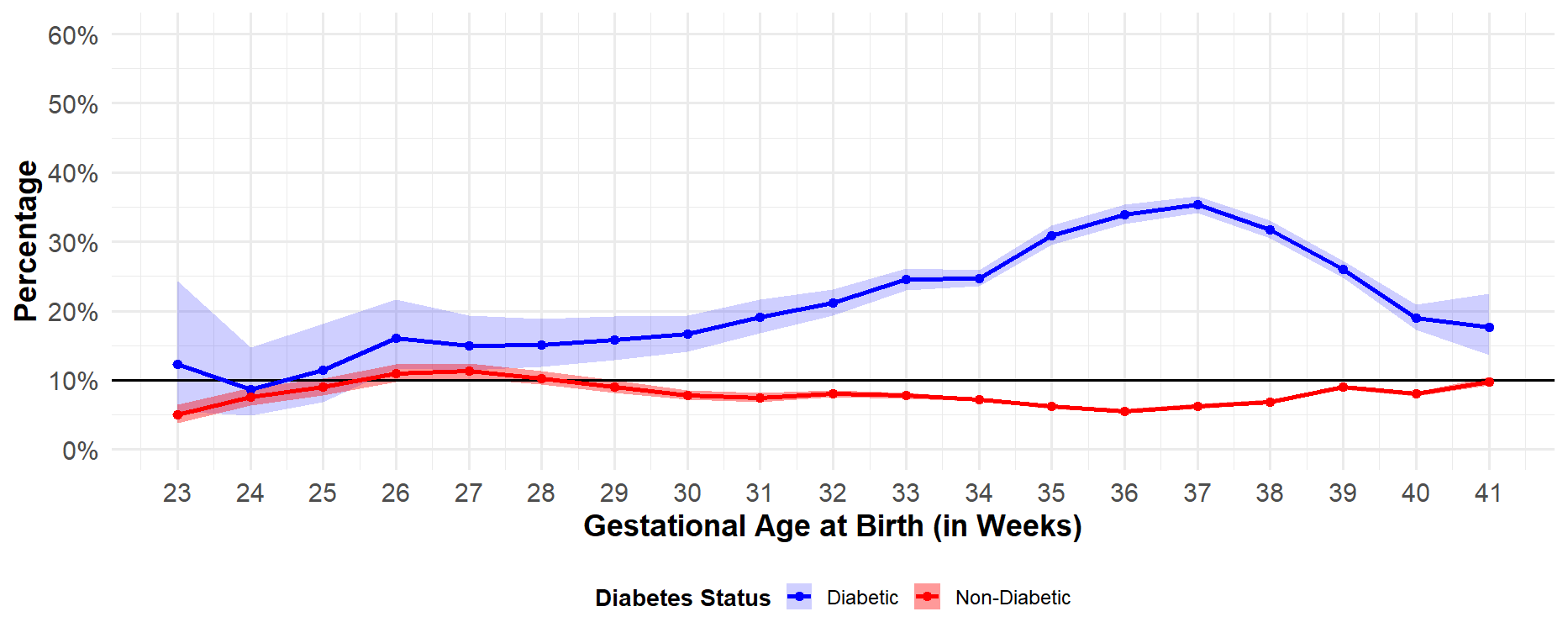
Background: Maternal conditions like diabetes, hypertensive disorders of pregnancy (HDP), and smoking are thought to impact infant size at birth, with infants of diabetic mothers at risk of high birthweight and infants of mothers with HDP or who smoke at greater risk of low birthweight. Infants born to mothers with these conditions are more likely to be born prematurely and may spend more time in the neonatal intensive care unit (NICU) for monitoring and treatment. Whether these maternal morbidities have similar effects on birth size by gestational age (GA) is not known. Objective: To determine the relationship between maternal diabetes, HDP and smoking with infant birthweight by GA. Design/Methods: Birth data from the Pediatrix Clinical Data Warehouse for singleton infants born at 23-41 weeks GA between 2013 and 2018 who were admitted to the NICU were analyzed (n=302,505). Birthweight was classified small (SGA, < 10th percentile), appropriate (AGA, 10th- 90th percentile), and large (LGA, > 90th percentile) for GA using the Olsen curves. Infants were stratified by maternal morbidity and GA. HDP included both pre-eclampsia and hypertension; maternal diabetes was not specific to type. The distribution of birthweight classification was reported for each maternal morbidity by GA with corresponding 95% confidence intervals. Results: Being born to a diabetic mother was associated with increased SGA at 24 weeks' GA (27.3%, 95% CI: [20.5%, 35.3%] diabetic vs. 17.4%, 95% CI: [15.7%, 19.2%] non-diabetic) but decreased SGA at later GAs (32-40 weeks; 4.6% to 8.1% diabetic vs. 7.9% to 15.6% non-diabetic). Conversely, LGA classification was more common among NICU infants of diabetic mothers at later GAs (28-41 weeks GA; 15.0% to 35.3% diabetic vs. 5.5% to 10.3% non-diabetic ). HDP was associated with a significant increase in SGA among NICU infants at all GAs (23-41 weeks; 13.1% to 52.0% HDP vs. 5.0% to 13.5% non-HDP), as well as LGA for infants born after 34-39 weeks (12.5% to 16.4% HDP vs. 9.2% to 10.9% non-HDP). Maternal smoking was associated with significantly increased SGA (11.9% to 22.0% smoker vs. 7.6% to 13.0% non-smoker) and decreased LGA (3.8% to 8.2% smoker vs. 8.8% to 12.6% non-smoker) only for infants born at 33 weeks or later.
Conclusion(s): The relationship between maternal morbidity with infant size varies by maternal condition and GA. While HDP associates with greater SGA at all GAs, smoking and diabetes are associated with smaller and larger birth size, respectively, only as infants approach term birth.
Percent of US NICU Infants with LGA Birthweight by Maternal Diabetes Status

 photo")