660 - Association of 2D measurements with ventricular volumes and neurodevelopmental outcomes
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2643.660
Daniela Salvo Sánchez, The Hospital for Sick Children, Toronto, ON, Canada; Ting Guo, The Hospital for Sick Children, Toronto, ON, Canada; Mehmet Cizmeci, The Hospital for Sick Children, Toronto, ON, Canada; Stephanie Au-Young, The Hospital for Sick Children, Toronto, ON, Canada; Linh G. Ly, The Hospital for Sick Children, Toronto, ON, Canada; Helen Branson, The Hospital for Sick Children, Toronto, ON, Canada; Edmond N. Kelly, University of Toronto Temerty Faculty of Medicine, Toronto, ON, Canada; Steven P,.. Miller, University of British Columbia Faculty of Medicine, Vancouver, BC, Canada; Vann Chau, The Hospital for Sick Children, Toronto, ON, Canada
Clinical fellow The Hospital for Sick Children Toronto, Ontario, Canada
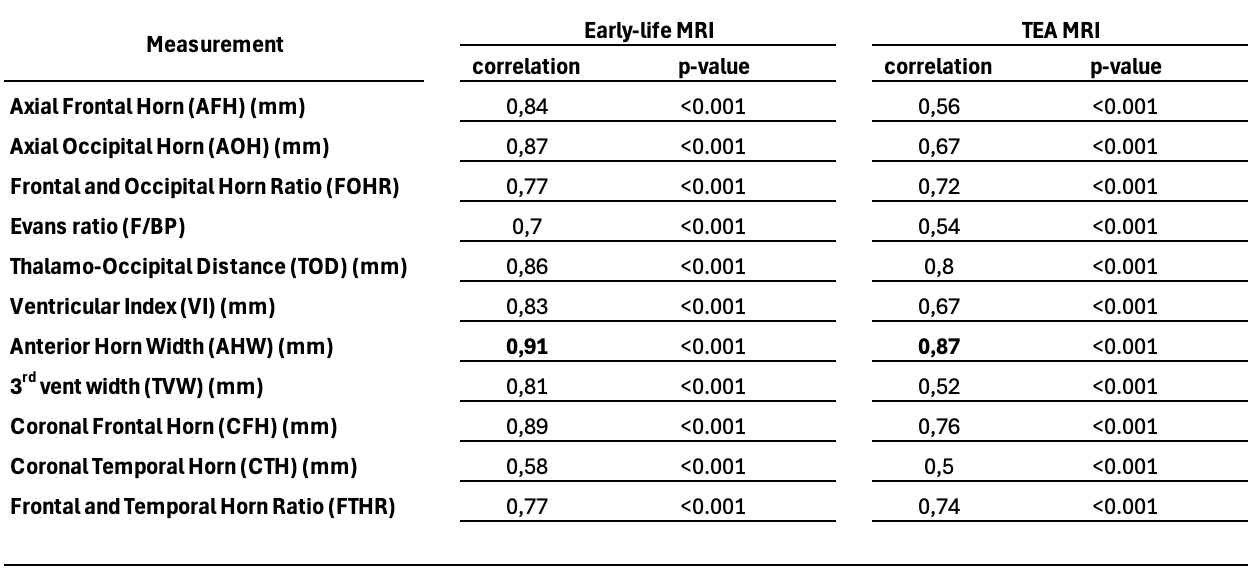
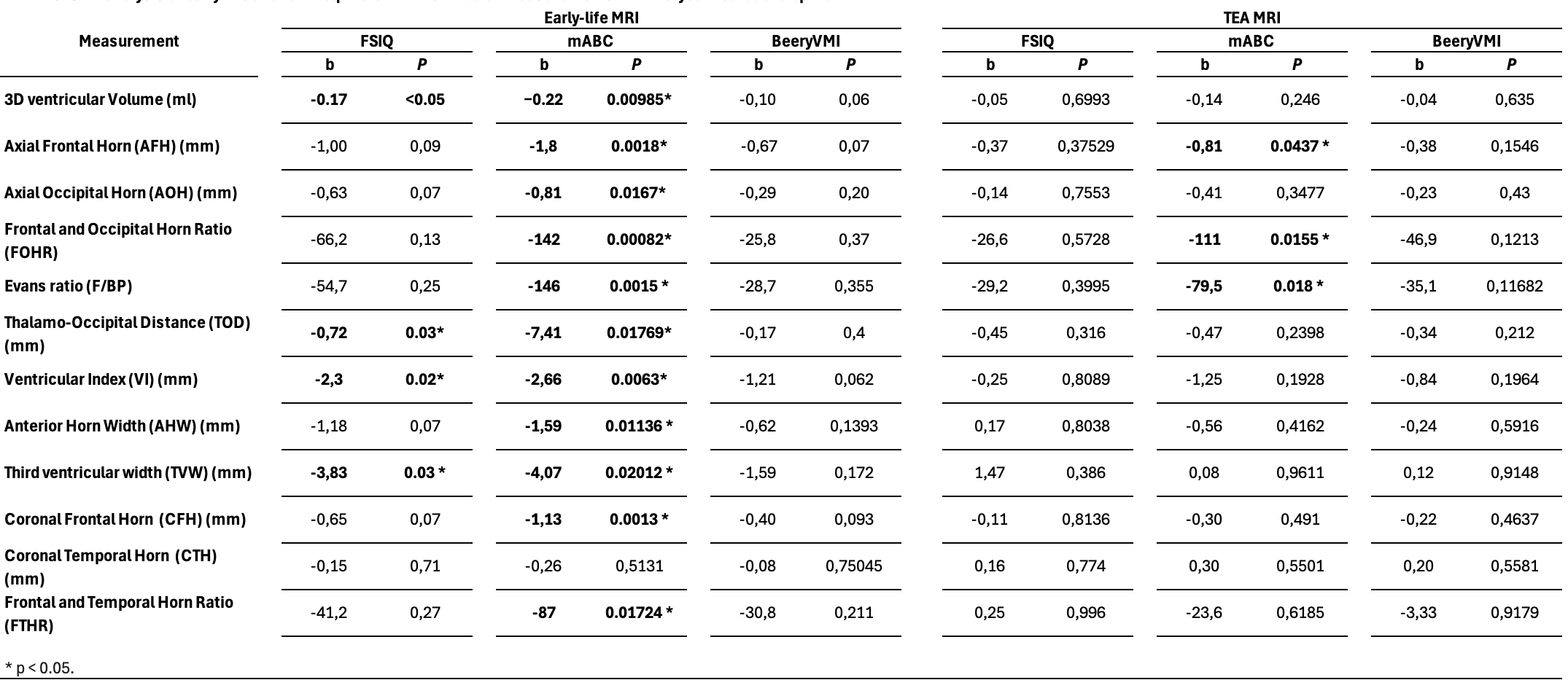
Background: Enlarged ventricles are a common brain abnormality in very preterm infants and linked to adverse neurodevelopmental outcomes. Several two-dimensional (2D) ventricular widths are measured clinically, yet their relationships with 3D ventricular volumes on neonatal MRI and with neurodevelopment remain unclear. Objective: (1) assess 2D ventricular widths at early-life and term-equivalent age (TEA) on PACS and how they correlate with 3D volumes, and (2) assess their association with neurodevelopmental outcomes at 4.5 years. Design/Methods: 195 Very preterm infants underwent early-life and/or TEA MRI. 2D ventricular widths and 3D volumes were obtained. Neurodevelopmental outcomes at 4.5 years were assessed using Wechsler Preschool and Primary Scale of Intelligence (WPPSI-IV), Movement ABC (MABC), and Beery Visual-Motor Integration (VMI). Pearson correlation between each 2D width and 3D volume was calculated. Generalized linear models (GLM) were applied to assess the association of each 2D width and 3D volume measured at each time point with neurodevelopmental outcomes at 4.5 years adjusting for birth gestational age, post-menstrual age at MRI, sex, white matter injury volume, severe intraventricular hemorrhage, and total cerebral volume (TCV). Results: All 2D widths (Table 1) showed moderate to very strong correlations with 3D volume (r > 0.5), with anterior horn width (AHW) at early life (r = 0.91) and at term age (r = 0.87) showing the strongest association (Table 2). Early-life thalamo-occipital distance (TOD: ß=-0.72, p=0.03), ventricular index (VI: ß=-2.30, p=0.02), third ventricle width (TVW: ß=-3.83, p=0.03), and 3D ventricular volume (ß=-0.0002, p< 0.05) were significantly associated with lower FSIQ scores, and 3D ventricular volume (ß=-0.22, p< 0.05) and all of the 2D widths (p < 0.03) except coronal temporal horn (CTH) were associated with MABC scores. At TEA, only axial frontal horn (AFH: ß=-0.81, p=0.04), frontal and occipital horn ratio (FOHR: ß=-111, p=0.02), and Evans ratio (ß=-79.50, p=0.02) were linked to poorer motor performance (Table 3).
Conclusion(s): 2D ventricular widths (TOD, VI, TVW) at early-life strongly correlate with 3D volumes and predict cognitive and motor outcomes at 4.5 years in very preterm infants beyond the severity of brain injury and TCV, suggesting the importance of early-life MRI in assessing ventricular size for predicting neurodevelopmental outcomes in very preterm infants.
Table 1: Summary of 2D and 3D measurements at early life and term-equivalent age
Table 2: Pearson correlations between 2D ventricular measurements and 3D ventricular volumes
Table 3: GLM analysis of early-life and term-equivalent 2D ventricular measurements with 4.5-year neurodevelopment


.png)