729 - Beyond Survival: Multisystem Health Outcomes in Extremely Preterm Infants at 2–5 Years of Age
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2711.729
ANU SACHDEVA, All India Insitute of Medical Sciences, New Delhi, New Delhi, Delhi, India; DEEPIKA KAINTH, All India Institute of Medical Sciences, New Delhi, New Delhi, Delhi, India; M JEEVA SANKAR, All India Institute of Medical Sciences, New Delhi, New Delhi, Delhi, India; RAMESH AGARWAL, All India Institute of Medical Sciences, New Delhi, New Delhi, Delhi, India; Ankit Verma, AIIMS, Delhi, Delhi, India
Additional Professor All India Insitute of Medical Sciences, New Delhi New Delhi, Delhi, India
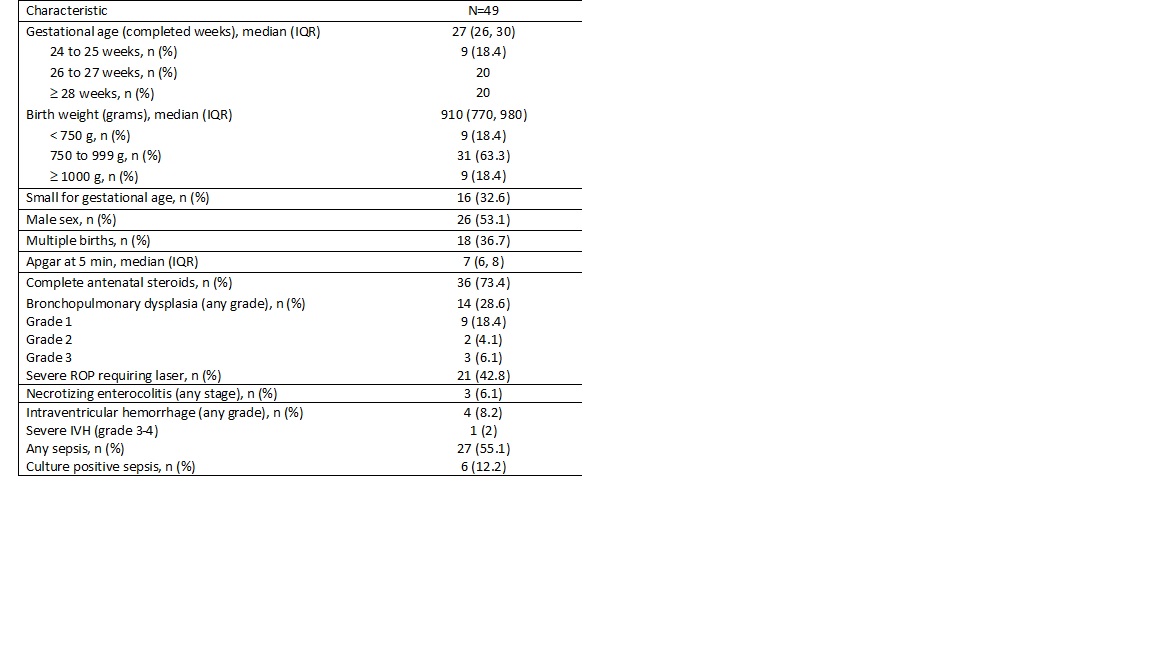
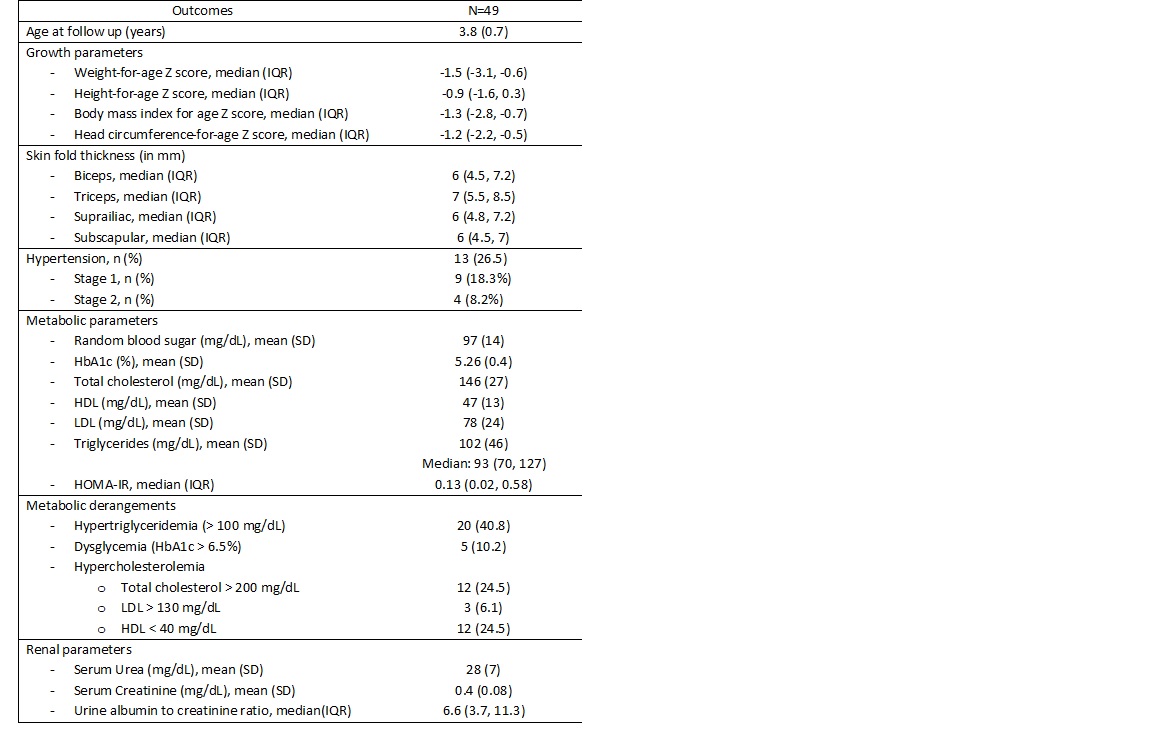
Background: There is enough data on the survival and short-term outcomes of extremely low gestational age and extremely low birth weight infants from low middle-income countries (LMICs). However, the data on childhood cardiometabolic outcomes remains scarce. Objective: To determine cardiometabolic outcomes among children aged 2 to 5 years born with a birth weight less than 1000 g or gestation less than 28 weeks. Additional objectives were to identify early renal and cardiovascular alterations suggestive of subclinical dysfunction. Design/Methods: Type of study: Cross-sectional study Setting: High-Risk Clinic, AIIMS, New Delhi. Inborn neonates with a birth weight less than 1000 g or gestation less than 28 weeks admitted to our NICU and being followed up in our high-risk clinic, and now in the age group 2 to 5 years were enrolled after obtaining informed parental consent. We measured weight and length/height according to WHO-MGRS protocols, then calculated "Z-score" for weight-for-age and height-for-age using the WHO Child Growth Standards in the WHO Anthro software. We assessed metabolic status through fasting glucose, insulin, HbA1c, lipid profile, and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR). We evaluated cardiovascular status by measuring blood pressure and carotid intima-media thickness (cIMT) using ultrasonography. We analysed the data using STATA 18.0 (StataCorp LLC. College station, TX) Results: A total of 49 children at 3.8 (±0.7) years were assessed. The median Z-scores for weight-for-age and BMI-for-age were -1.5 and -1.3, respectively. The gestation and birth weight were 27 (IQR 26 to 30) wks and 910 (770-980) g respectively. Nearly one-third (16/49) were small for gestational age, and 14/49 (28.6%) had bronchopulmonary dysplasia (Table 1). Hypertension was detected in 13/49 (26.5%). Mean HbA1c was 5.26%, while 5/ 49 children (10%) showed dysglycemia (HbA1c > 6.5%) and 20 (41%) had hypertriglyceridemia. (Stage 1: 18.3%; Stage 2: 8.2%). Serum LDL was 78 ± 24 mg/dL, and serum 47 ± 13 mg/dL. However low HDL ( < 40 mg/dL) was observed in 12/49 (24%). Median urine albumin/creatinine ratio was 6.6 (IQR 3.7 to 11.3), with normal serum creatinine (Table 2)
Conclusion(s): Children born extremely low birth weight have a high prevalence of hypertension, dysglycemia and hypertriglyceridemia. These findings underscore the need for structured long-term multidisciplinary follow-up programs and early preventive interventions in this high-risk group to mitigate lifelong health risks.
Table 1. Baseline characteristics of the cohort at discharge during the birth hospital stay
Table 2. Cardiometabolic outcomes at 2-5 years of age

 photo")