131 - Eltrombopag plus immunosuppressive therapy versus immunosuppressive therapy alone for pediatric severe aplastic anemia: a systematic review and meta-analysis.
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2126.131
Filippo Furlanetto, University of Bologna, Bologna, Emilia-Romagna, Italy; Candela Lang, University of Miami, Miami, FL, United States; Isabela Hartmann Rost, Federal University of Health Sciences of Porto Alegre (UFCSPA), Porto Alegre, Rio Grande do Sul, Brazil; Letícia Rocha Campos, University of Ribeirao Preto, Ribeirão Preto, Sao Paulo, Brazil; Nourah Almarri, Al jahra hospital, Ardiya, Al Farwaniyah, Kuwait; Maria A.. Torres, Universidad Tecnológica de Pereira, Cali, Valle del Cauca, Colombia
Medical Student University of Bologna Bologna, Emilia-Romagna, Italy
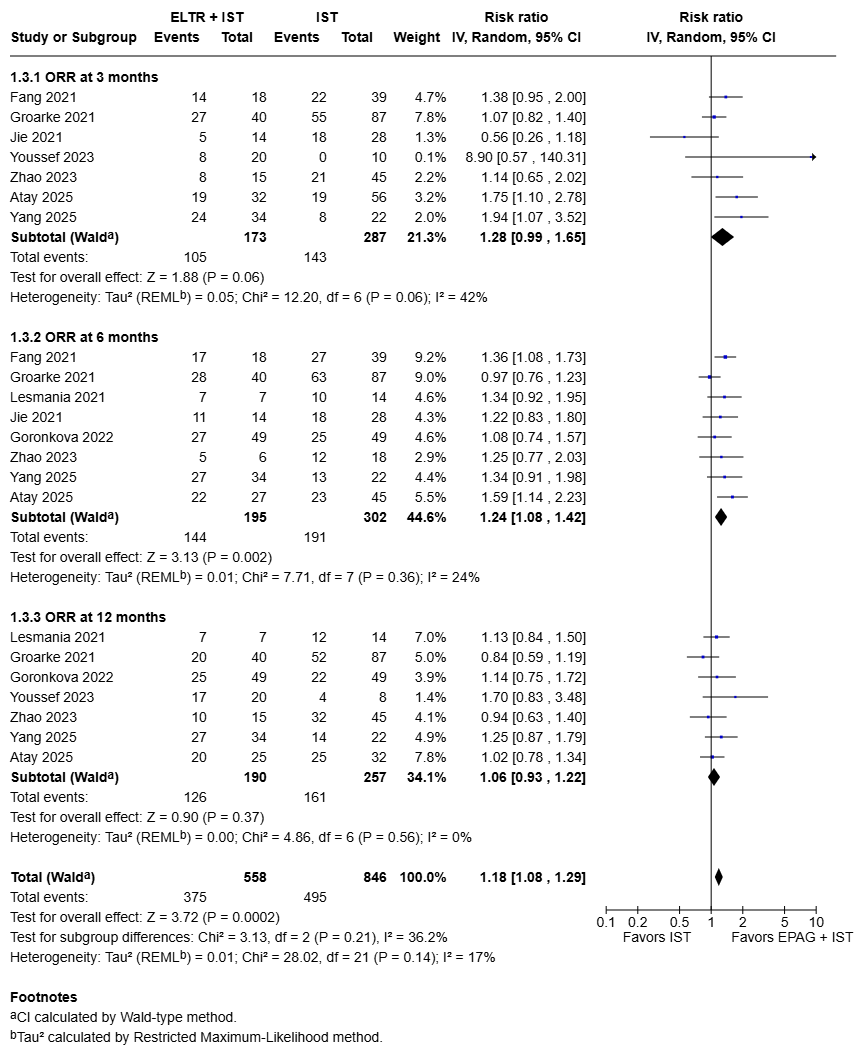
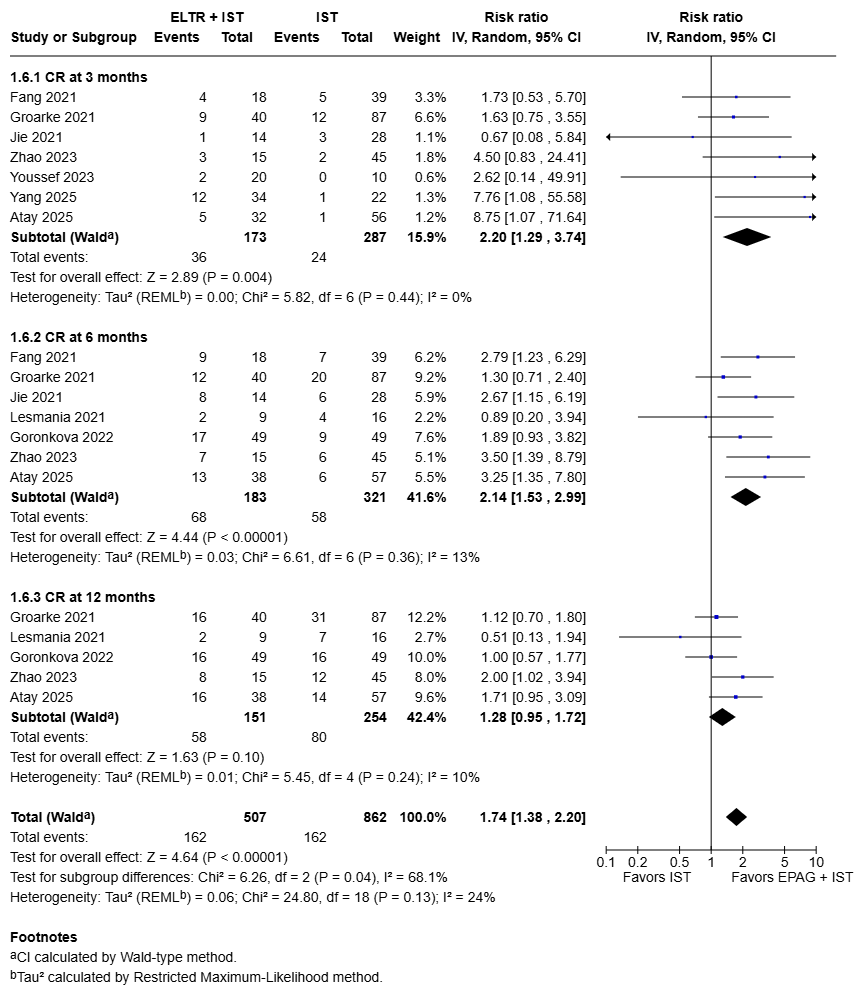
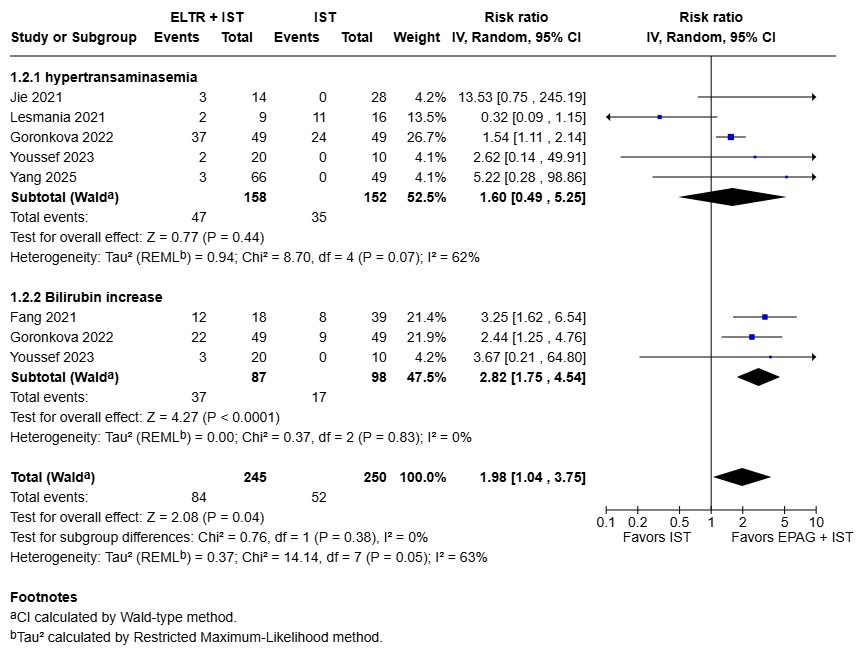
Background: Severe aplastic anemia (SAA) is a rare but life-threatening hematologic emergency affecting 2-3 children per million annually. It is characterized by profound pancytopenia with rapid progression to fatal complications. Matched sibling donor (MSD) hematopoietic stem cell transplantation remains the standard of care; however, only 25-30% of patients have an available donor. For the remaining majority, immunosuppressive therapy (IST) with antithymocyte globulin (ATG) plus cyclosporine is the standard first-line treatment. Eltrombopag (EPAG), a thrombopoietin receptor agonist, has improved outcomes in adult SAA, but its benefit in pediatric populations remains uncertain. Objective: To evaluate the safety and efficacy of Eltrombopag plus IST versus IST alone in pediatric patients with severe aplastic anemia without a matched sibling donor. Design/Methods: Following PRISMA guidelines, a systematic search of MEDLINE, Embase, and Cochrane databases was conducted through October 2025. Randomized and observational studies were included. Primary outcomes were overall response rate (ORR) and complete response (CR) at 3, 6, and 12 months post-treatment; secondary outcomes included hepatotoxicity. Statistical analysis was performed using RevMan 5.4. Results: Nine studies (total n = 649) met inclusion criteria: 269 (41.4%) received EPAG+IST and 380 (58.6%) received IST alone. ORR improved over time with EPAG+IST: a near-significant trend at 3 months (RR 1.28; 95% CI 0.99-1.65; p=0.06), significant benefit at 6 months (RR 1.24; 95% CI 1.08-1.42; p = 0.002), and no difference by 12 months (RR 1.06; 95% CI 0.93-1.22; p = 0.37). CR showed marked early improvement at 3 months (RR 2.20; 95% CI 1.29-3.74; p = 0.004) and persisting at 6 months (RR 2.14; 95% CI 1.53-2.99; p < 0.00001), converging by 12 months (RR 1.28; 95% CI 0.95-1.72; p = 0.10). Safety analysis revealed increased bilirubin elevation with EPAG+IST (RR 2.82; 95% CI 1.75-4.54; p < 0.0001), and no significant difference in hypertransaminasemia occurred (RR 1.60; 95% CI 0.49-5.25; p = 0.44).
Conclusion(s): Adding Eltrombopag to standard IST accelerates early hematologic recovery and more than doubles the chance of complete response during the first 6 months, when the risk of bleeding and infection is greatest. By 12 months response rates converge, and the safety profile remains acceptable, with mild, reversible bilirubin elevations. These findings support eltrombopag as a safe, effective first-line strategy for the majority of pediatric SAA patients lacking MSD, while highlighting the need for larger prospective trials to confirm long‑term benefits.