34 - Factors Associated with Developmental Dysplasia of the Hip Among Neonates Born at Elmhurst Hospital
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2031.34
Amrita Suresh, Icahn School of Medicine at Mount Sinai/Elmhurst, Elmhurst, NY, United States; Helly Thakkar, Icahn School of Medicine at Mount Sinai, Rego park, NY, United States; Chaithanya Avanthika, Icahn School of Medicine at Mount Sinai, New York City, NY, United States; Uday P.. Patil, Icahn School of Medicine at Mount Sinai-NYC H+H-Elmhurst, Elmhurst, NY, United States; Jennifer L. Pintiliano, Icahn School of Medicine at Mount Sinai, Elmhurst, NY, United States
Pediatric Resident Physician Icahn School of Medicine at Mount Sinai/Elmhurst Elmhurst, New York, United States
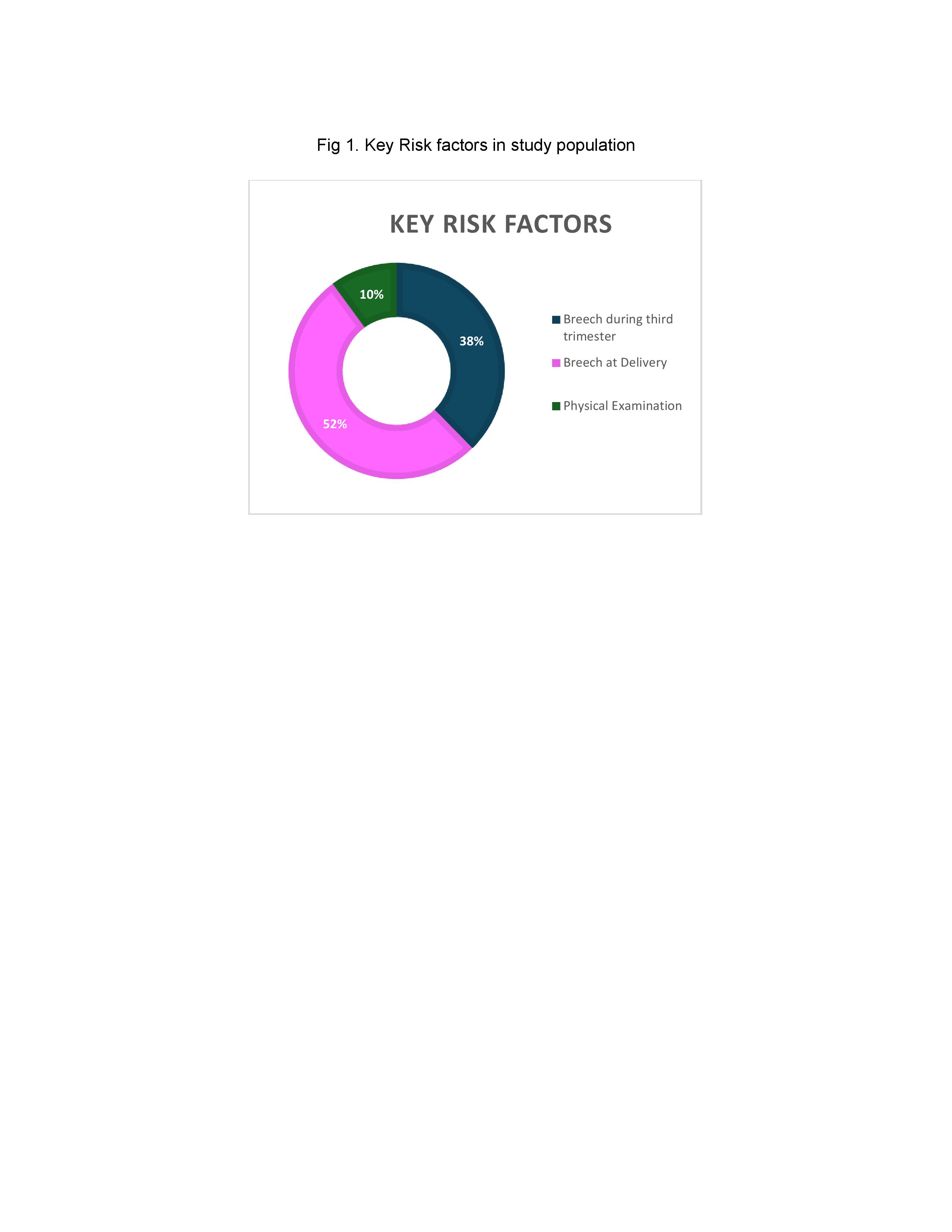
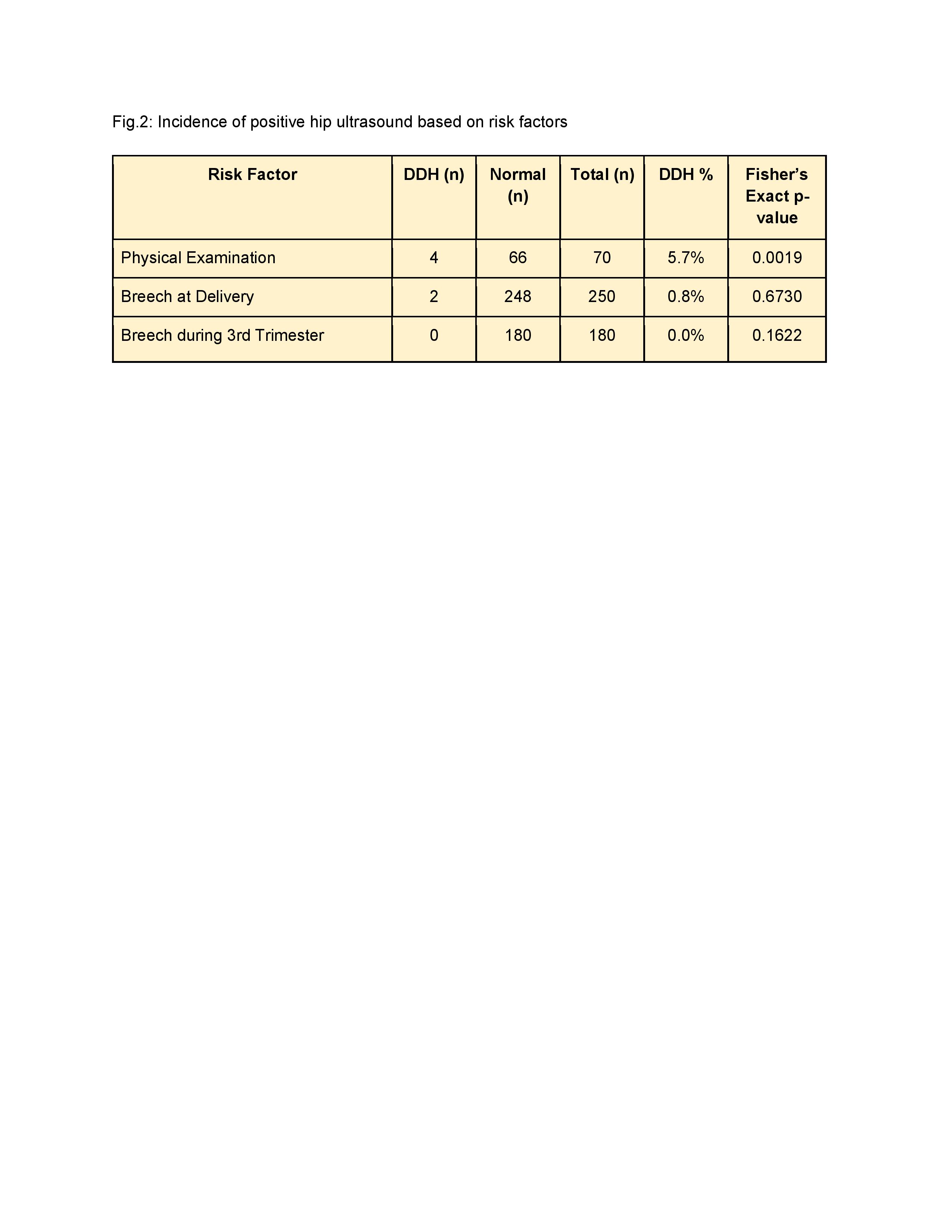
Background: Developmental dysplasia of the hip (DDH) occurs in approximately 1 in 1000 live births. Selective DDH screening remains debated due to limited consensus in the literature supporting the American Academy of Pediatrics (AAP) guidelines from 2000. According to these guidelines, newborns with positive physical findings or high-risk features, such as breech presentation, are referred for hip ultrasonography at six weeks of age. Recent studies suggest that breech positioning at any point during the third trimester, rather than at delivery, is a more critical factor in DDH development. Objective: This study evaluates the incidence of DDH and associated risk factors in neonates at Elmhurst Hospital to inform future screening practices. Design/Methods: A retrospective chart review was conducted on 547 neonates referred for hip ultrasound screening at Elmhurst Hospital between May 2020 and May 2024. Patient records were accessed via the EPIC system. Inclusion criteria required documented indications for referral and completed sonographic imaging. Exclusions included, suboptimal imaging, missing referral indication, or infants not born at our hospital. Data collected included referral indications, ultrasound results, and physical exam findings at the time of referral. Statistical analysis was performed using SAS, and Chi-Square tests assessed associations between risk factors and DDH diagnosis. Results: Of the 547 neonates screened, 478 were included, 5 cases (1.05 %) were diagnosed with DDH. Common referral indications included breech delivery (52.30%), breech positioning in the third trimester (37.66%), and positive physical exam findings (10.04%). A significant association was found between positive physical exams and DDH (p < 0.0001). However, neither breech positioning in the third trimester nor breech delivery was significantly associated with DDH. Among the 69 excluded, 2 with DDH had positive physical examination findings but were not born at our hospital. Fisher's exact test confirmed the strong correlation between positive physical exams and DDH (p < 0.0001).
Conclusion(s): This study reinforces the predictive value of a positive physical exam in identifying DDH, whereas breech positioning in the third trimester was not a significant indicator. Breech presentation at delivery yielded two positive results but was not statistically significant. These findings support the continued importance of clinical assessment in DDH screening. Tailoring screening practices to focus on more predictive risk factors could improve outcomes and resource utilization in newborn care.
Fig.1: Key risk factors in study population
Fig.2: Incidence of positive hip ultrasound based on risk factors

.jpg "Amrita Suresh, MD (she/her/hers) photo")