355 - Outcomes of Infants with Procedural Complications or Failure of Less Invasive Surfactant Administration in the Neonatal Intensive Care Unit
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2344.355
Savanah Gallegos, Los Angeles General Medical Center, Agoura Hills, CA, United States; japmeet sandhu, Kaiser, Denair, CA, United States; Sheryar Siddiqui, CHOC Children's Hospital of Orange County, Orange, CA, United States; Emilio Feliz Sala, Keck School of Medicine of the University of Southern California, Los Angeles, CA, United States; Amy Yeh, USC/Los Angeles General Medical Center, Los Angeles, CA, United States; Hemananda Muniraman, Los Angeles General Medical Center, Los Angeles, CA, United States; Manoj Biniwale, Cedars Sinai Medical Center, Los Angeles, CA, United States
Resident Physician Los Angeles General Medical Center Agoura Hills, California, United States
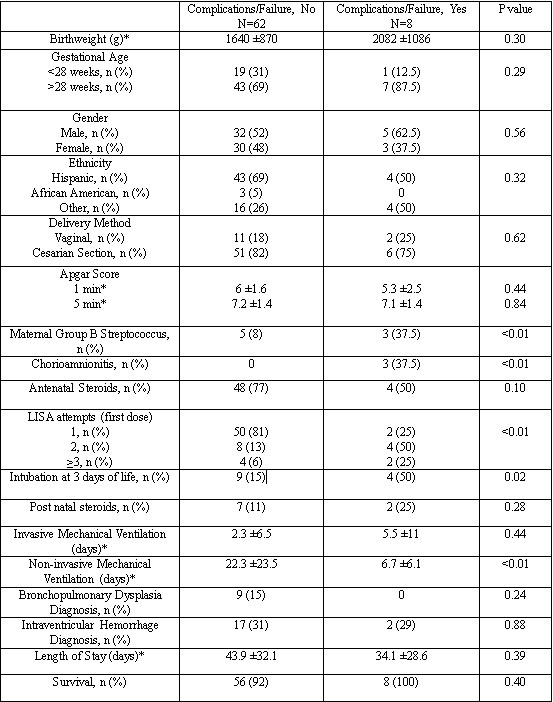
Background: Less Invasive Surfactant Administration (LISA) is a widely utilized technique in the neonatal intensive care unit (NICU) in which a thin catheter is used to deliver surfactant. LISA has been associated with improved neonatal outcomes of bronchopulmonary dysplasia (BPD) and intraventricular hemorrhage (IVH), as well as less mechanical ventilation. However, procedure-related complications associated with LISA include desaturations, bradycardia, need for positive pressure ventilation, and improper placement of the catheter. Objective: The purpose of this study is to determine factors affecting complications or failure of LISA and their outcomes. Design/Methods: This was a retrospective cohort study (2020-2024) of 70 infants admitted to a Level III NICU at Los Angeles General Medical Center who received surfactant via LISA. Maternal and neonatal demographics were collected from the electronic NICU database and electronic medical records. Infants were grouped into those with and without procedure-related complications (desaturations, bradycardia, need for positive pressure ventilation) or failure. Chi square test was used to determine differences in categorical variables, and T test was used to analyze continuous variables. Results: There were 70 infants included in this study; 8 patients experienced complications or failure with LISA and 62 did not. Infant demographics were similar between the two groups. There were no differences in delivery method or Apgar scores between the two groups. A higher percentage of those who experienced complications were exposed to maternal group B streptococcus (p < 0.01) and chorioamnionitis (p < 0.01). Surfactant doses administered via LISA were similar in both groups. A higher percentage of infants who experienced procedure-related complications required invasive mechanical ventilation at 3 days of life (p=0.02) but spent less time on non-invasive mechanical ventilation (p < 0.01). There were no differences in outcomes of BPD, IVH, length of stay, home oxygen use, or survival.
Conclusion(s): Procedure-related complications with LISA were associated with short-term outcomes of need for invasive mechanical ventilation at 3 days of life, though no long-term pulmonary comorbidities. Chorioamnionitis and maternal group B streptococcus were seen in higher rates in those with procedure-related complications, likely due to perinatal stress.
Demographics and outcomes of patients with procedural complications or failure of Less Invasive Surfactant Administration *Mean ±Standard Deviation

 *Mean ±Standard Deviation
*Mean ±Standard Deviation