56 - Utilizing Swallow Studies in the Level III NICU to Facilitate Safe Discharge Home
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2053.56
Pamela Dodrill, Brigham and Women's Hospital, Boston, Boston, MA, United States; Samuel Chutkow, Carleton College, Needham, MA, United States; Katherine A.. Gibson, Brigham and Women's Hospital, Boston, Exeter, NH, United States; Carmina Erdei, Brigham and Women's Hospital and Harvard Medical School, Boston, MA, United States; Helen Christou, Harvard Medical School, Boston, MA, United States
Clinical specialist - NICU feeding therapy team Brigham and Women's Hospital, Boston Boston, Massachusetts, United States
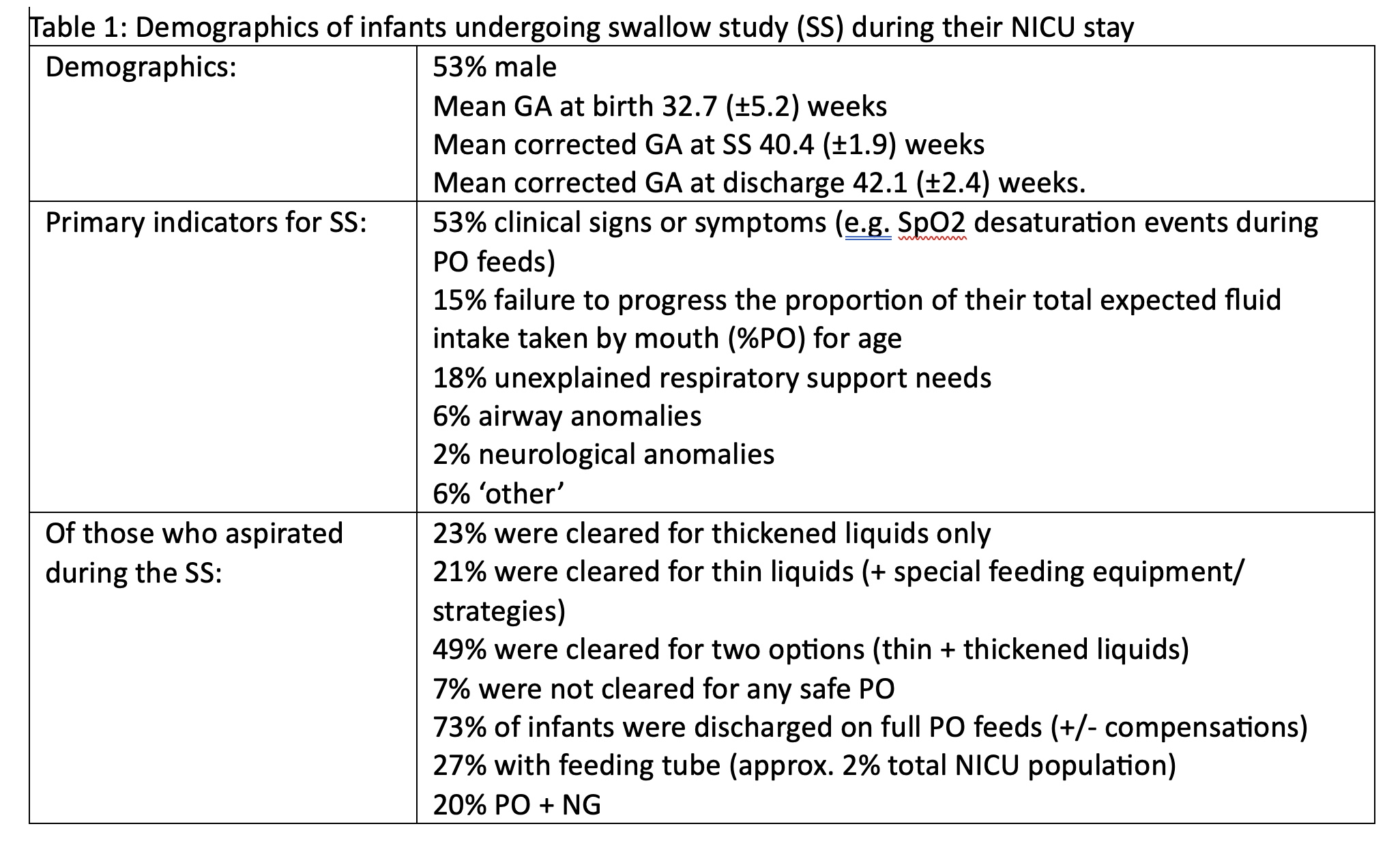
Background: Most preterm infants admitted the Neonatal Intensive Care Unit (NICU) initially rely on nasogastric (NG) tube feeds and gradually transition to oral (per os, PO) feeds. Some medically-complex infants do not achieve independent PO feeding by their due date; this is generally related to degree of prematurity and severity of illness. Feeding problems in the NICU are often related to immature suck-swallow-breath coordination, and silent aspiration is relatively common. The American Academy of Pediatrics recommends that standard neonatal care includes availability of swallow studies to evaluate aspiration risk, either on-site or with established policies to facilitate neonatal transfer to a higher level of care. Objective: Describe population characteristics for NICU infants who undergo swallow studies (SS) and their feeding outcomes. Design/Methods: A retrospective chart review was conducted for neonates admitted ≥72 hours to a level III urban, academic center NICU with on-site availability of SS over a 3-year period (2022-2025). IRB approval was obtained. Descriptive statistics (mean ± SD and %) relating to feeding outcomes are reported. Results: On average, 820 infants were admitted per annum (pa), and 747pa were discharged home from the NICU. Of these, 11% received a SS during their NICU stay (n=247, 82pa). See Table 1. Among infants who underwent SS, 59% were found to be aspirating. An additional 26% were discharged with a complex feed plan (e.g. home tube feeds/ respiratory support). Most infants who were found to be aspirating on SS still achieved full PO feeds by around their due date (41.0 +/- 2.9 weeks corrected GA) with necessary compensations in place (e.g. thickened liquids, special bottle nipples). Outpatient follow-up SS were performed in 35% of infants who underwent a SS in the NICU (mean 30.1 ± 17.3 days post-discharge), and 71% were cleared to liberalize their feed plan.
Conclusion(s): Feeding problems in the NICU population are relatively common, and often related to immature suck-swallow-breath coordination. More than half of infants who undergo SS in the NICU are found to be aspirating, but most can go home feeding PO, with appropriate compensations and ongoing support. Specialized neonatal speech pathology services and access to SS in a level III NICU are essential to accurately characterize swallowing physiology and aspiration risk, and help guide safe feeding plans for high-risk hospitalized infants.
Demographics of infants undergoing swallow study (SS) during their NICU stay