36 - Maximum versus Mean Transcutaneous Bilirubin Level: Which Screens Best?
Retrospective analysis of prospectively collected triplicate transcutaneous bilirubin measurements
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2033.36
Frouke J. Terpstra, University Medical Center Groningen, Groningen, Groningen, Netherlands; Lauren EH. Westenberg, Erasmus MC, Rotterdam, Zuid-Holland, Netherlands; Peter H. Dijk, Childrens, Groningen, Groningen, Netherlands; Elisabeth M.W.. Kooi, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, Groningen, Netherlands; Jasper V. Been, Erasmus MC Sophia Children's Hospital, Rotterdam, Zuid-Holland, Netherlands; Christian V. Hulzebos, Beatrix Children's Hospital, University Medical Center Groningen, Groningen, Groningen, Netherlands
PhD-Candidate University Medical Center Groningen Groningen, Groningen, Netherlands
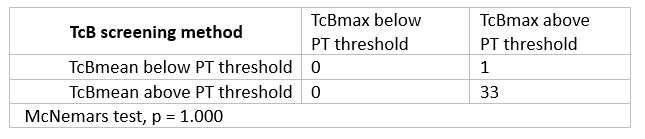
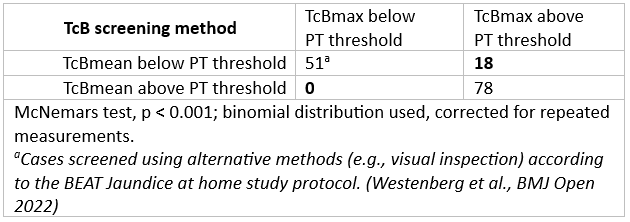
Background: Transcutaneous bilirubin (TcB) measurements, with an added safety margin, are a reliable, non-invasive screening method for early detection of jaundiced neonates who need phototherapy (PT). Usually, the result of three successive TcB measurements determines whether quantification of total serum bilirubin (TSB) is needed. However, it is not well studied if the mean (TcBmean) or maximum (TcBmax) of this triplicate measurement is more accurate and safe in identifying neonates who need PT. We hypothesized that using TcBmax would decrease the likelihood of missing newborns who require treatment, although it might increase the number of unnecessary heel pricks for TSB quantification. Objective: To assess whether TcBmax versus TcBmean more accurately identifies neonates requiring phototherapy, and if its use affects the number of unnecessary heel pricks. Design/Methods: Data were derived from the Dutch prospective multi-cohort BEAT Jaundice at Home study. In this cohort of 2314 (near)term neonates, TSB quantification was performed only when indicated by clinical parameters, including TcB measurements with the Dräger JM-105 (Dräger, Lübeck, Germany). We included a subset of whom three TcB measurements and a TSB were recorded at the same time. McNemar's tests were used to compare TcBmax and TcBmean in either identifying neonates with a TSB above or below the PT threshold. Defining the latter as 'unnecessary heel pricks'. Results: Data from 181 TcB measurements in 152 neonates were analyzed with a median [IQR] gestational age of 38 [37-39] weeks and mean (SD) birthweight of 3316grams (460). All neonates were in the low (n=121, 80%) or in the medium (n=31, 20%) PT threshold risk group. The median TSB was 225 µmol/L [193-273], the median difference between TcBmax and TcBmean was 10 µmol/L 5-16]. Table 1 shows that 34 (22%) neonates had a TSB above the PT threshold. Of these, one neonate was only identified by TcBmax (NS, p=1.000). Table 2 shows that 147 (81%) TSB measurements were below the PT threshold, 78 (43%) were cases where either TcB led to a TSB measurement. Using TSBmax led to an additional 18 (10%) unnecessary heel pricks versus TcBmean (p < 0.001). The sensitivity of TcBmax and TcBmean for detecting TSB levels above the PT threshold was 100% and 97%, respectively (McNemar test, NS), while specificity was 34.7% and 46.9%, respectively (McNemar test, χ² = 16.06, p < 0.001).
Conclusion(s): In the home-care setting, TcBmax may identify more neonates qualifying for phototherapy than TcBmean, but at the cost of significantly more blood sampling.
Table 1. Number of TcB measurements with a TSB above PT threshold (n=34).
Table 2. Number of TSB measurements below the PT threshold (n=147), identified as unnecessary heel pricks.