347 - A Novel Diuretic and Steroid Protocol for Patients with Bronchopulmonary Dysplasia
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2336.347
Grace A. Hooker, University of Texas at Austin Dell Medical School, Austin, TX, United States; Sheena John, Dell Children's Medical Center of Central Texas, Austin, TX, United States; Jianzhong Ji, Dell children's Medical center, cedar park, TX, United States
Medical Student University of Texas at Austin Dell Medical School Austin, Texas, United States
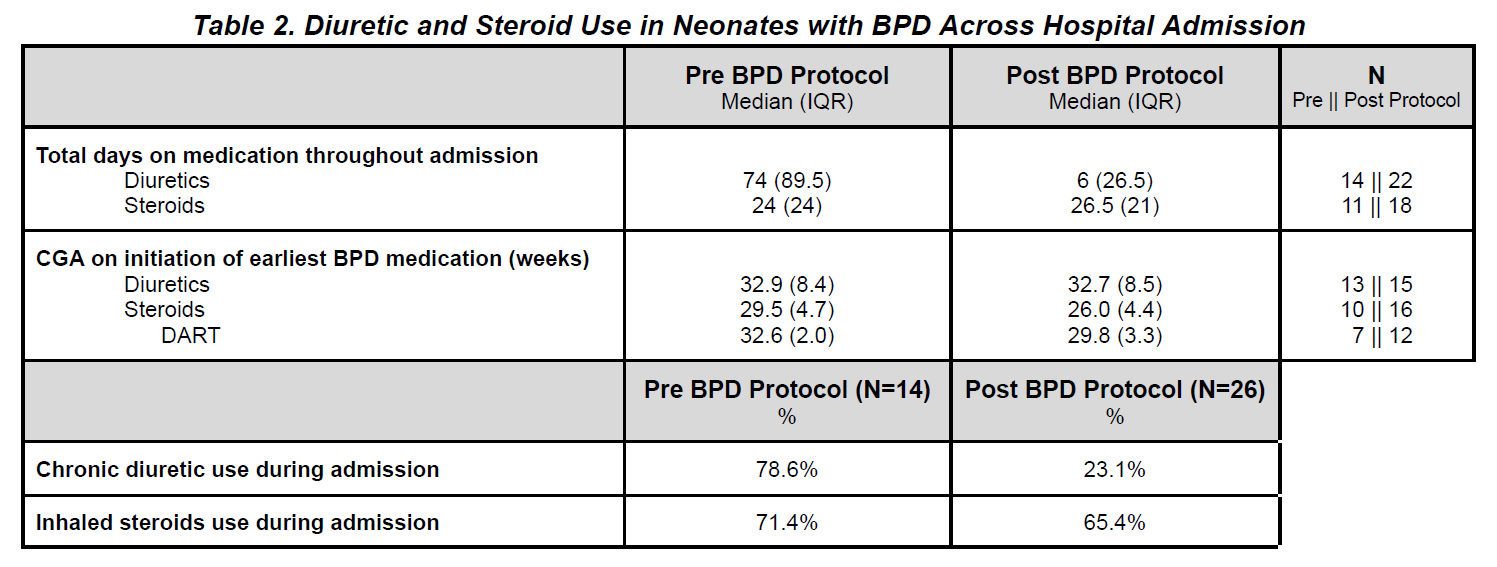
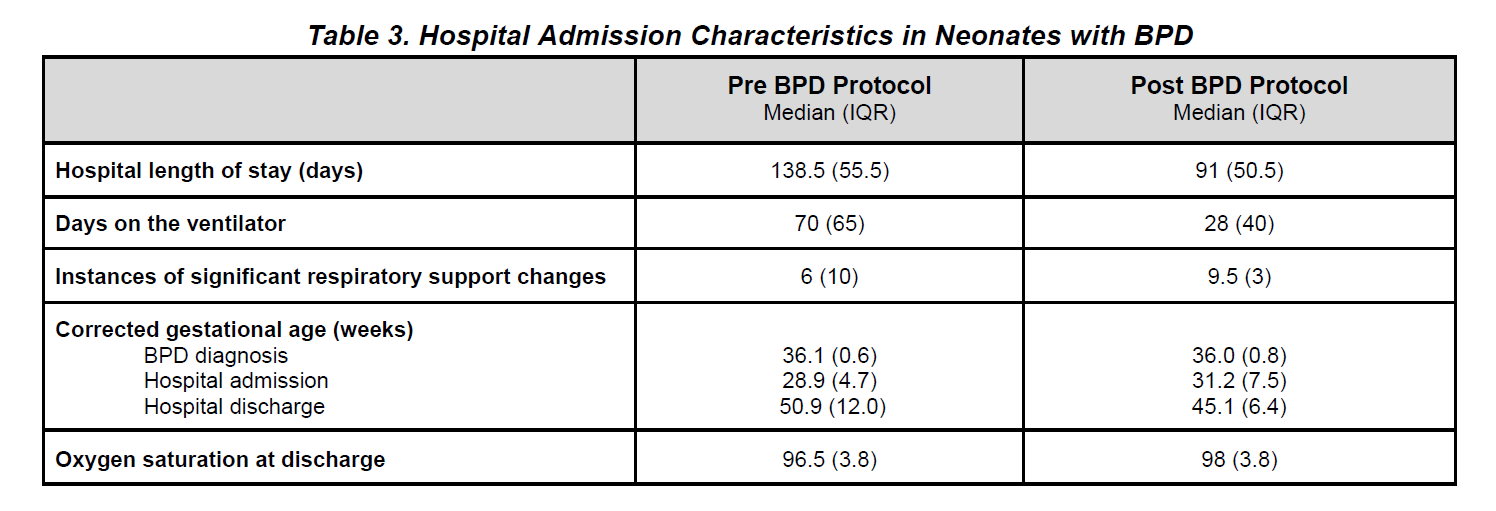
Background: Bronchopulmonary dysplasia (BPD) remains a major cause of morbidity among preterm infants, with wide variation in corticosteroid and diuretic use across neonatal intensive care units (NICUs). Lack of standardized guidance on medication selection, dosing, and duration may contribute to inconsistent outcomes and adverse effects. Objective: To evaluate whether implementation of a novel steroid and diuretic protocol, which provides clinical guidance on optimal medication selection, dose, and duration, reduces medication utilization among infants with BPD in a tertiary NICU. Primary outcomes were total steroid and diuretic utilization. Secondary outcomes were BPD severity and respiratory status at discharge, days on ventilator, and length of stay. Design/Methods: This retrospective cohort study included 40 infants with mild/grade 1, moderate/grade 2, or severe/grade 3 BPD admitted between Jan. 2022 and Mar. 2025. Infants with respiratory disease not primarily due to BPD were excluded. 14 infants comprised the pre-protocol group (1/2022-5/2023) and 26 comprised the post-protocol group (6/2023-3/2025). Results: After protocol implementation, median diuretic days declined from 74 days (pre) to 6 days (post) (Table 2). Median days of steroid exposure was 24 days (pre) and 26.5 days (post) (Table 2). 78.6% of the pre group met definition of chronic diuretic use, as defined as daily diuretic after a 3-5 day course or 2+ single days of diuretic, while 23.1% of the population in the post group met definition of chronic diuretic use. Pre-protocol neonates had a median of 70 days on ventilator support compared to a median of 28 days on ventilator support (post). Similarly, the hospital median length of stay for the pre-protocol group was 138.5 days, and the median length of stay for the post-protocol group was 91 days.
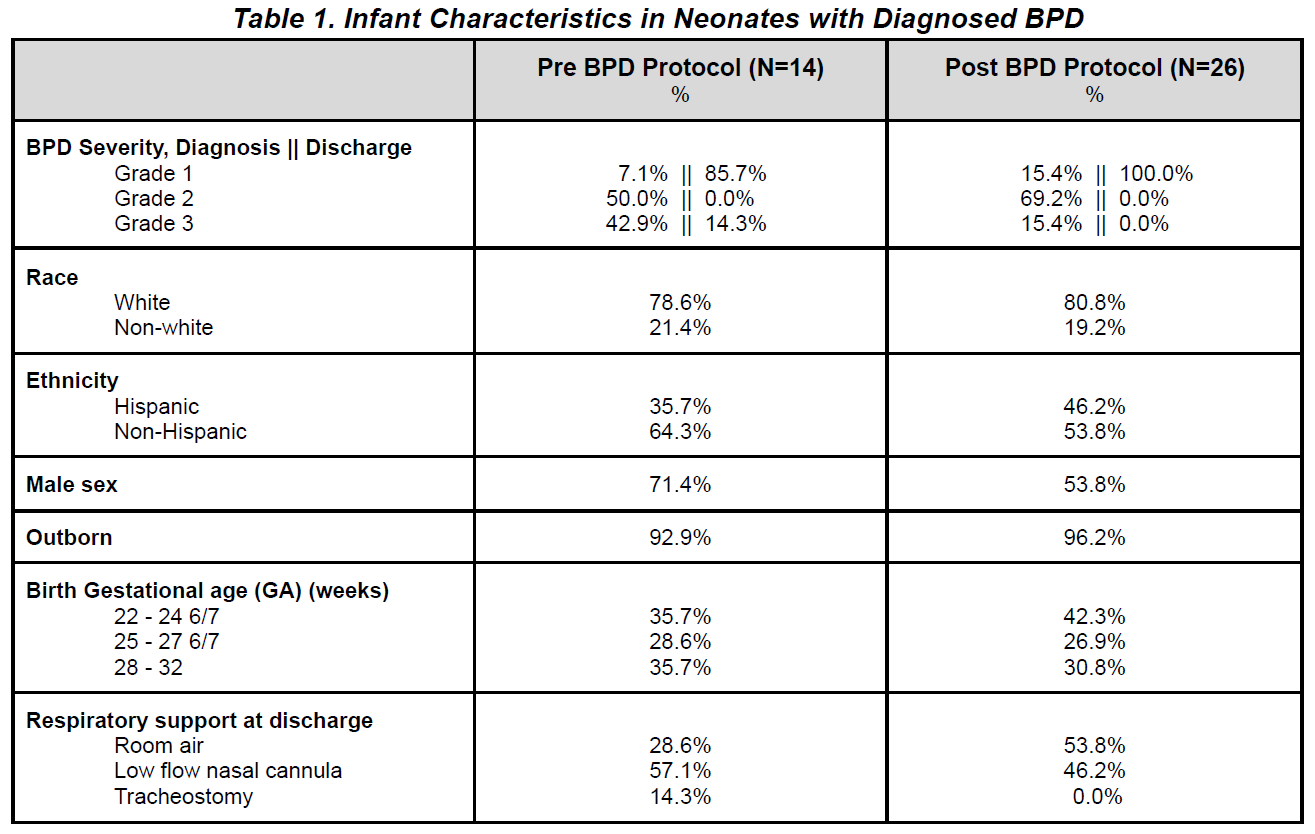
At diagnosis 50% and 42.9% of (pre) neonates had grade 2 and 3 BPD respectively, while 69.2% and 15.4% of (post) neonates had grade 2 and 3 BPD. At discharge 85.7% of (pre) neonates had grade 1 BPD, while 100% of (post) neonates had grade 1 BPD. Upon discharge, 57.1% and 28.6% of the (pre) group was discharged on low flow nasal cannula (LFNC) and room air (RA) respectively, while 46.2% and 53.8% of the (post) group was discharged on LFNC and RA.
Conclusion(s): Implementation of a standardized steroid and diuretic protocol was associated with reduced diuretic use, consistent prescribing practices, and stable respiratory outcomes. These findings support the feasibility of protocolized management and highlight the need for larger, multicenter studies to assess long-term safety and efficacy.
Table 1. Infant Characteristics in Neonates with Diagnosed BPD
Table 2. Diuretic and Steroid Use in Neonates with BPD Across Hospital Admission
Table 3. Hospital Admission Characteristics in Neonates with BPD

 photo")