525 - Optimizing the Prediction of Deep Musculoskeletal Infection Using Preliminary Clinical and Laboratory Values
Saturday, April 25, 2026
3:30pm - 5:45pm ET
Publication Number: 2510.525
Evan Wright, University of Texas Southwestern Medical School, Dallas, TX, United States; Lawson A.. Copley, UT Southwestern, Dallas, TX, United States; Norman A. Lapin, Scottish Rite for Children, Dallas, TX, United States; Naureen G.. Tareen, Children's Health Dallas, Dallas, TX, United States
Pediatric Emergency Physician University of Texas Southwestern Medical School Dallas, Texas, United States
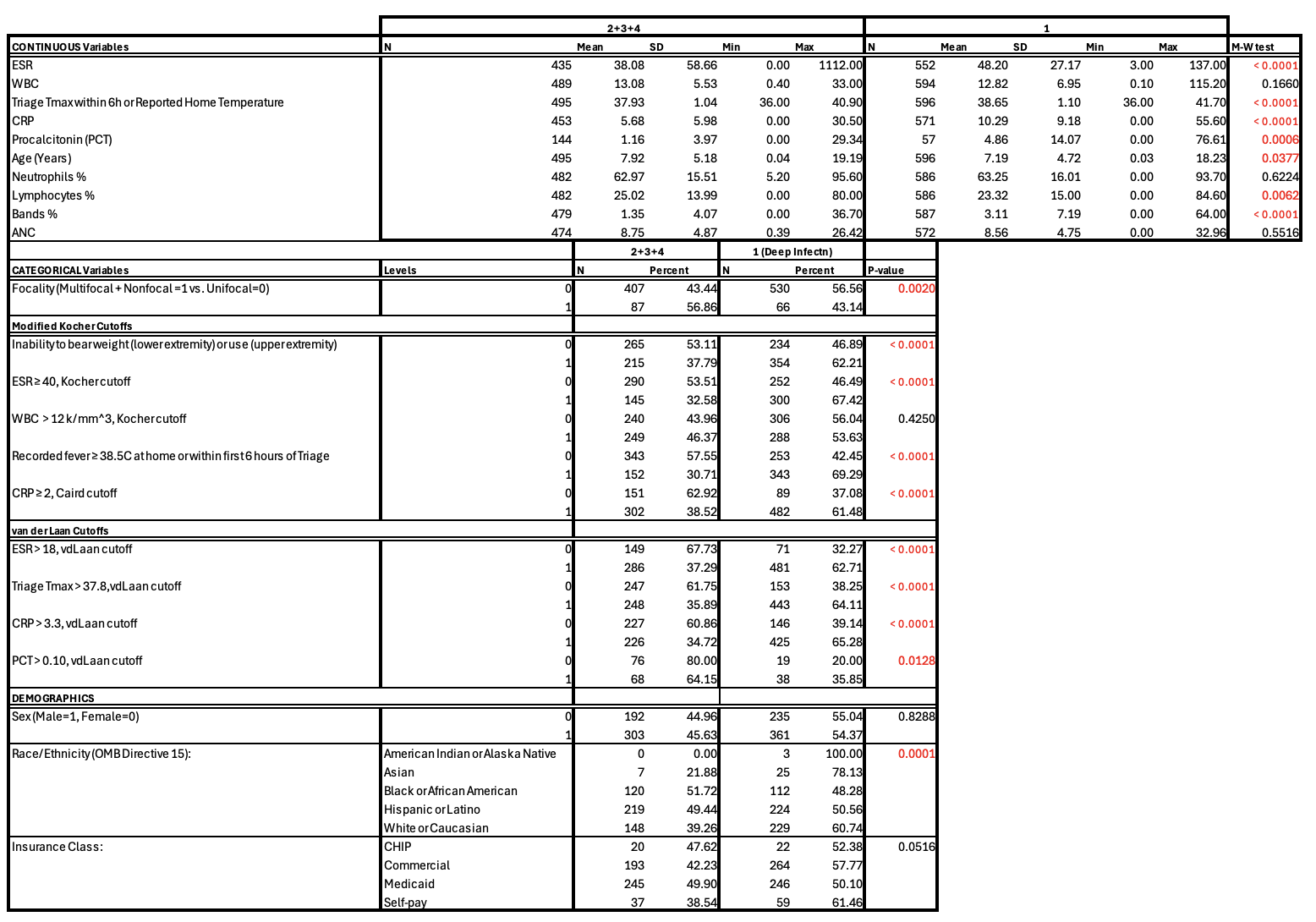
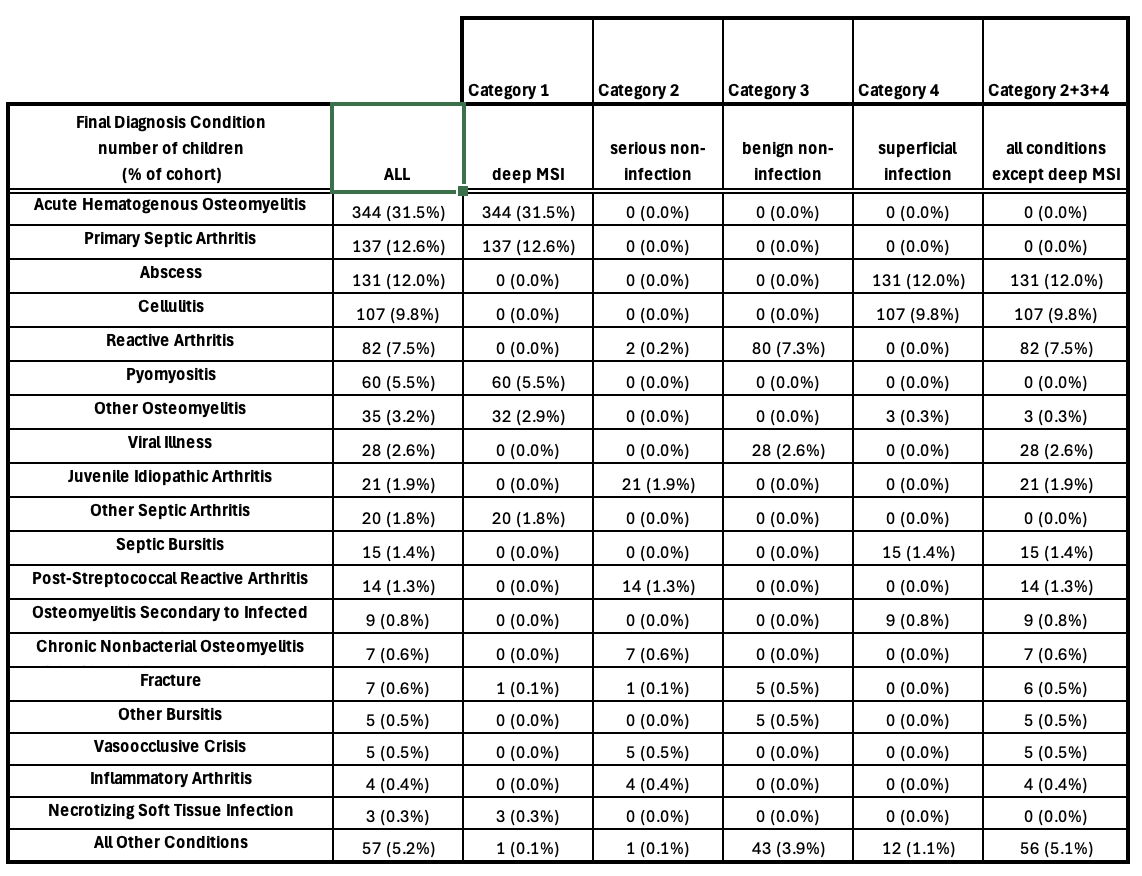
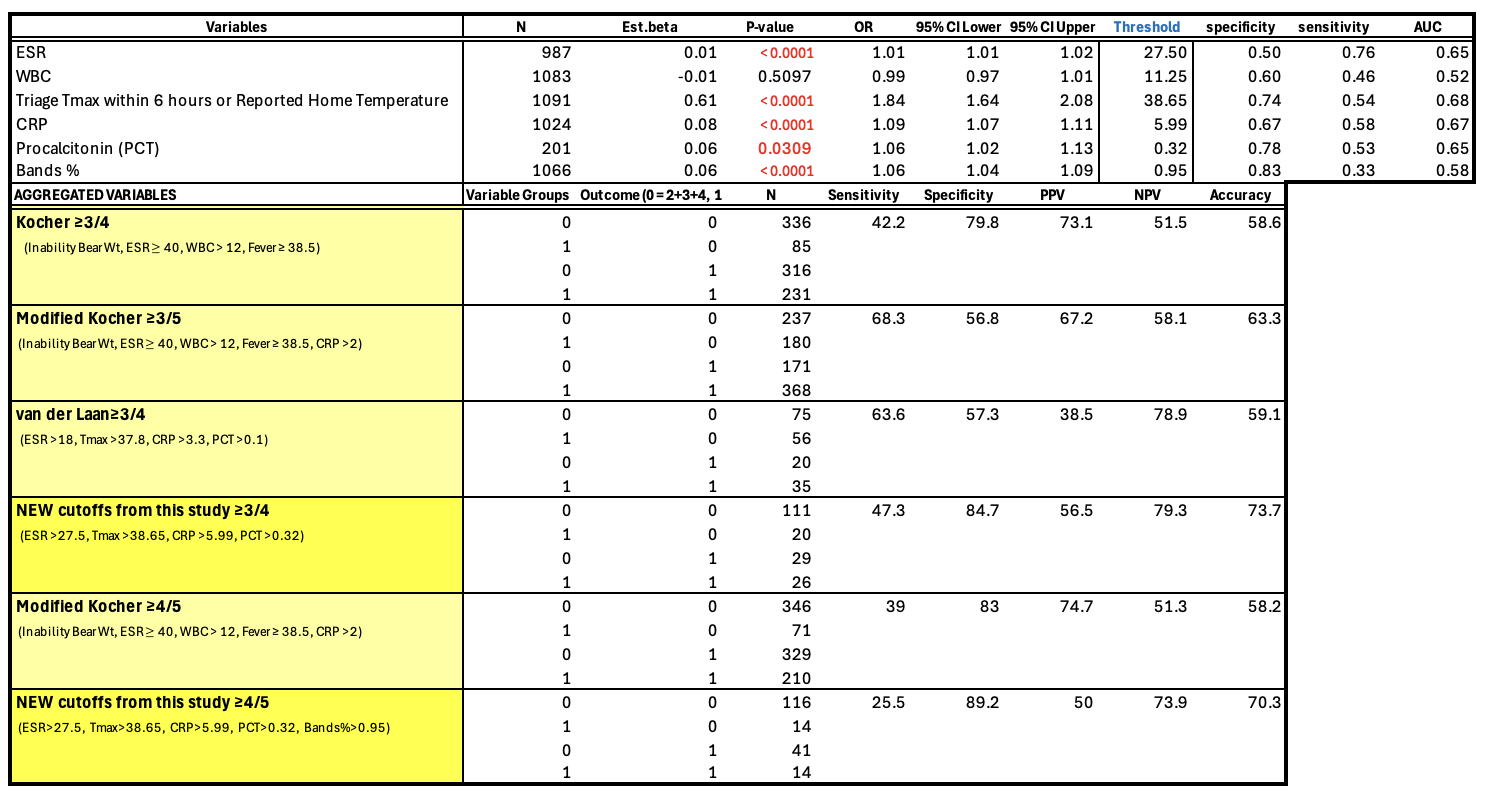
Background: In children, deep musculoskeletal infections (MSI)-including osteomyelitis, septic arthritis, and pyomyositis-pose significant morbidity risks and present diagnostic challenges in the acute setting. Previously proposed clinical prediction algorithms have notable limitations, including small sample sizes, limited external validation, focus on single-joint involvement, and omission of newer biomarkers such as procalcitonin (PCT). Objective: To validate previously studied predictive criteria using a larger, more comprehensive cohort and to propose a novel predictive algorithm for diagnosing deep MSI in children. Design/Methods: An IRB-approved retrospective chart review was conducted of 1,091 children admitted to a tertiary pediatric medical center from 2010-2023 with orthopedic consultation for suspected deep MSI. Final diagnoses were classified into four groups: 1) deep MSI, 2) non-infection (serious), 3) non-infection (benign), and 4) superficial infection. For statistical analysis, groups 2-4 were combined. Univariate analysis using Mann-Whitney and Receiver Operating Characteristic (ROC) analysis was performed. Diagnostic performance metrics were calculated for individual and combined variables. Results: Of the 1091 children, 596 (54.6%) were diagnosed with deep MSI. Compared with groups 2-4, significant predictors included inability to bear weight or use the affected limb (P < 0.0001), unifocal (P = 0.0020), ESR (48.2 ± 27.2 mm/hr vs. 38.1 ± 58.7 mm/hr, P < 0.0001), CRP (10.29 ± 9.18 mg/dL vs. 5.68 ± 3.30 mg/dL, P < 0.0001), PCT (4.86 ± 14.07 ng/mL vs. 1.16 ± 3.97 ng/mL, P = 0.0006), and band % (3.11% ± 7.19% vs. 1.35% ± 4.07%, P < 0.0001). WBC count did not differ significantly (12.82 × 10³/mm³ ± 6.95 vs. 13.08 × 10³/mm³ ± 5.53, P = 0.1660). New diagnostic cutoffs were identified as ESR > 27.5 mm/hr, temperature > 38.65 °C, CRP > 5.99 mg/dL, and PCT > 0.32 ng/mL. Using these thresholds, specificity, PPV, and accuracy improved to 84.7%, 56.5%, and 73.7% respectively, compared to 57.3%, 38.5%, and 59.1% using van der Laan criteria.
Conclusion(s): This study represents the largest analysis of pediatric deep MSI to date. Findings suggest WBC count, a component of previous prediction rules, may not be a useful biomarker for deep MSI. The Modified Kocher Criteria demonstrated substantially lower predictive probabilities than previously reported (93.1% and 97.5%). A revised predictive model using new biomarker thresholds shows improved diagnostic performance and may enhance early identification of pediatric deep MSI.
Comparison of continuous and categorical variables between children with and without deep MSI
Frequency distribution of final diagnoses among children evaluated for deep MSI
Univariate logistric regression for optimal diagnostic threshold and comparison of existing and newly derived predictive algorithms for diagnosing deep MSI