192 - A Quality Improvement Project to Reduce Open Encounters in a Large Academic Resident Continuity Clinic
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3184.192
Tomitra Latimer, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Nina L. Alfieri, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Natasa D.. Van Grinsven, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Lexi Artman, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Annette Calixto-Logan, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Preethi Raghupatruni, Lurie, Chicago, IL, United States
Interim Division Head Ann & Robert H. Lurie Children's Hospital of Chicago Chicago, Illinois, United States
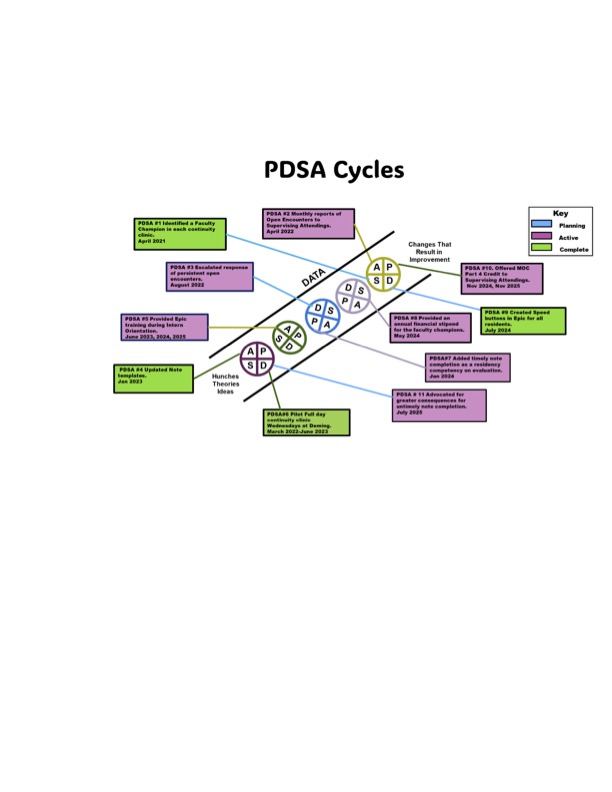
Background: Delayed note completion can impact patient safety, timely billing, and compliance with documentation standards. Our large urban academic pediatric division has two primary care clinic sites that host faculty practice sessions and 15 weekly continuity clinic (CC) sessions for 116 residents. Timely chart closure in CC has been a longstanding problem, attributed to multiple factors including competing resident's clinical and inpatient duties, electronic medical record inefficiencies, and preceptor delays in chart closing. In 2021, physician leaders and administrators launched a quality improvement (QI) project to address this issue. Objective: To reduce the number of open encounters in resident continuity clinics by 50% through a longitudinal QI initiative. Design/Methods: Fishbone and Key Driver Diagrams identified key drivers and barriers to timely note closure. Baseline data were collected to inform interventions. The initial SMART Aim of a 25% reduction was expanded to 50% due to early progress. Interventions included: 1. appointing and incentivizing a faculty champion in each clinic session to encourage timely chart closure among residents and preceptors 2. distributing monthly open encounter reports to supervising faculty to promote accountability, 3. developing concise user friendly note templates. Monthly team meetings reviewed open encounter data and trends, guiding subsequent (Plan-Do-Study-Act) PDSA interventions. Results: During the QI project, the average visit volume was 976 visits per month (range 929-1056). In November 2021, baseline open encounters totaled 183, peaking at 336 in 2022. By August 2025, following multiple PDSA cycles, open encounters declined to 37 total (an 80% reduction), with sustained improvement. (Figure 2). Faculty champions were the key driver of improvements, promoting accountability among residents and supervising attendings.
Conclusion(s): Through a QI approach emphasizing faculty champion leadership, monthly reporting and reminders, and note redesign, our clinics achieved a marked and sustained reduction in open encounters in resident continuity clinics. Remaining challenges include maintaining faculty engagement, improving the function and efficiency of EMR, and enforcing consistent consequences for open encounters. Ongoing efforts include evaluating the financial impact of note closure, continued adjustments to support sustained success, and protecting incentive funding for faculty champions. This QI project highlights that the elevation of the faculty champion can improve timely note closure and accountability.

 Credit")
 photo")