716 - Variation in imaging modality for pediatric nasal injury across children’s hospital emergency departments
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3693.716
Alexandria Georgadarellis, Boston Children's Hospital, Wayland, MA, United States; Michael Monuteaux, Boston Children's Hospital, Boston, MA, United States; Ingrid Ganske, Boston Children's Hospital, Boston, MA, United States; Mark Neuman, Harvard Medical School, boston, MA, United States; Andrew F. Miller, Boston Children's Hospital, Brookline, MA, United States
Assistant Physician Boston Children's Hospital Wayland, Massachusetts, United States
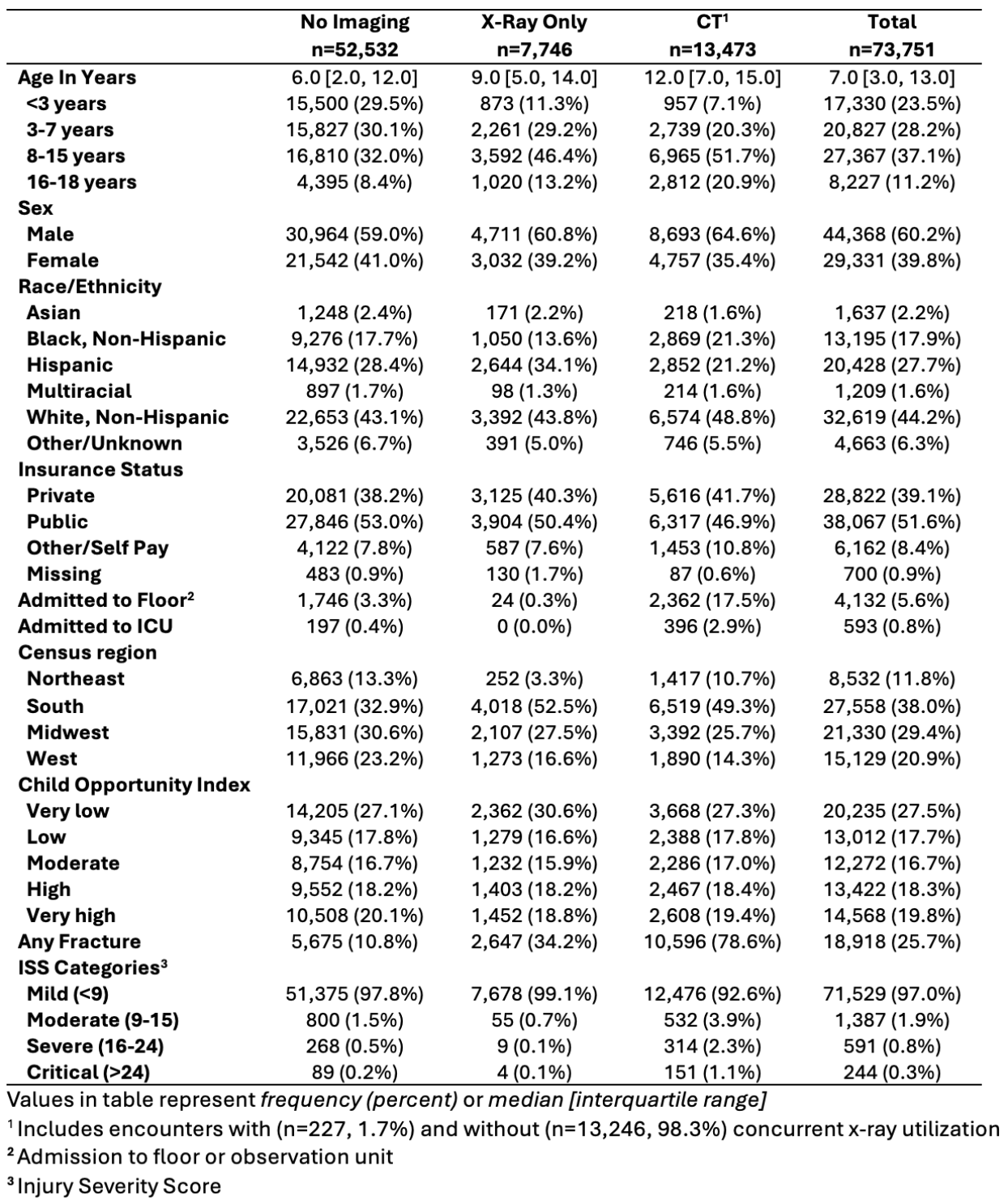
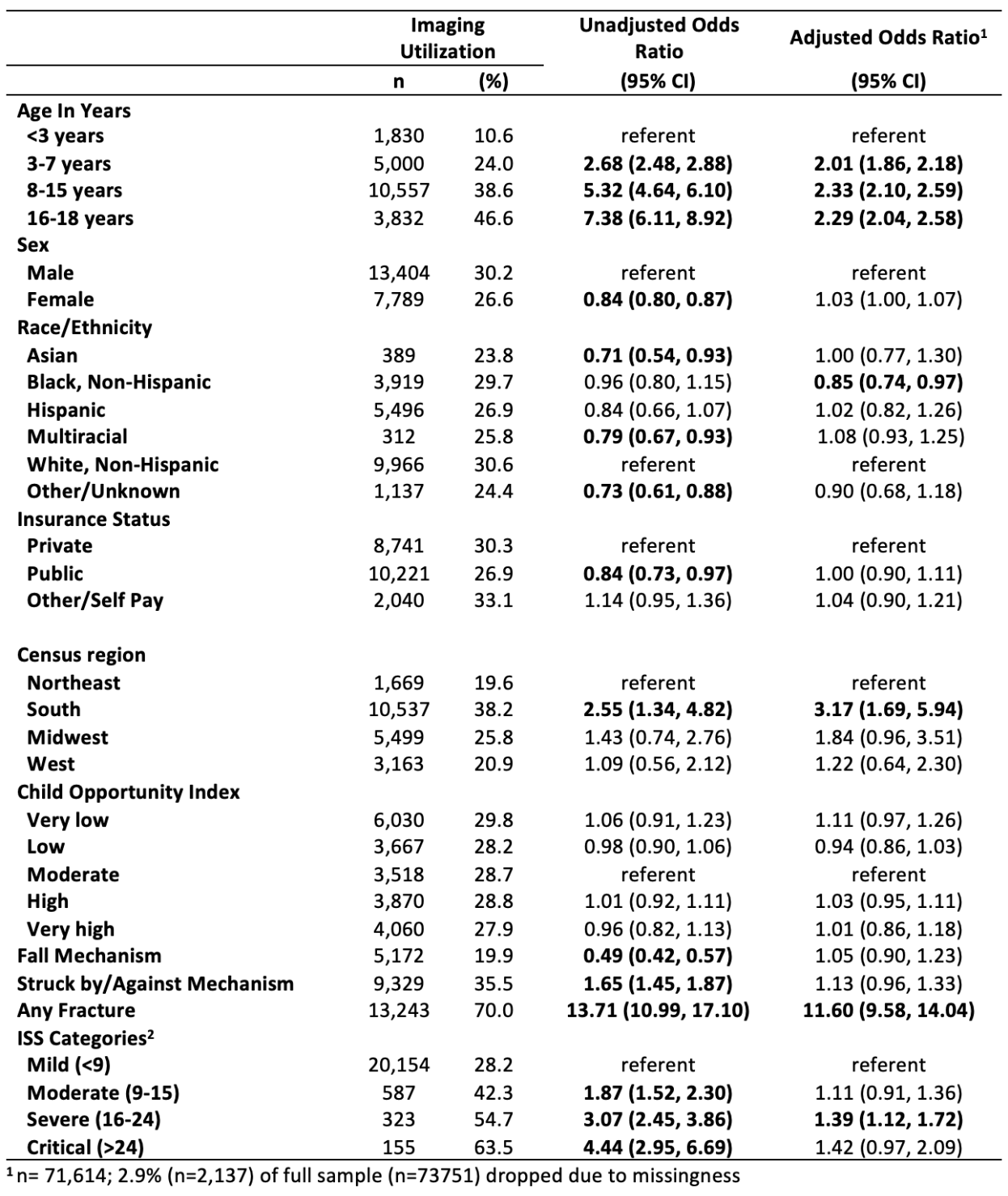
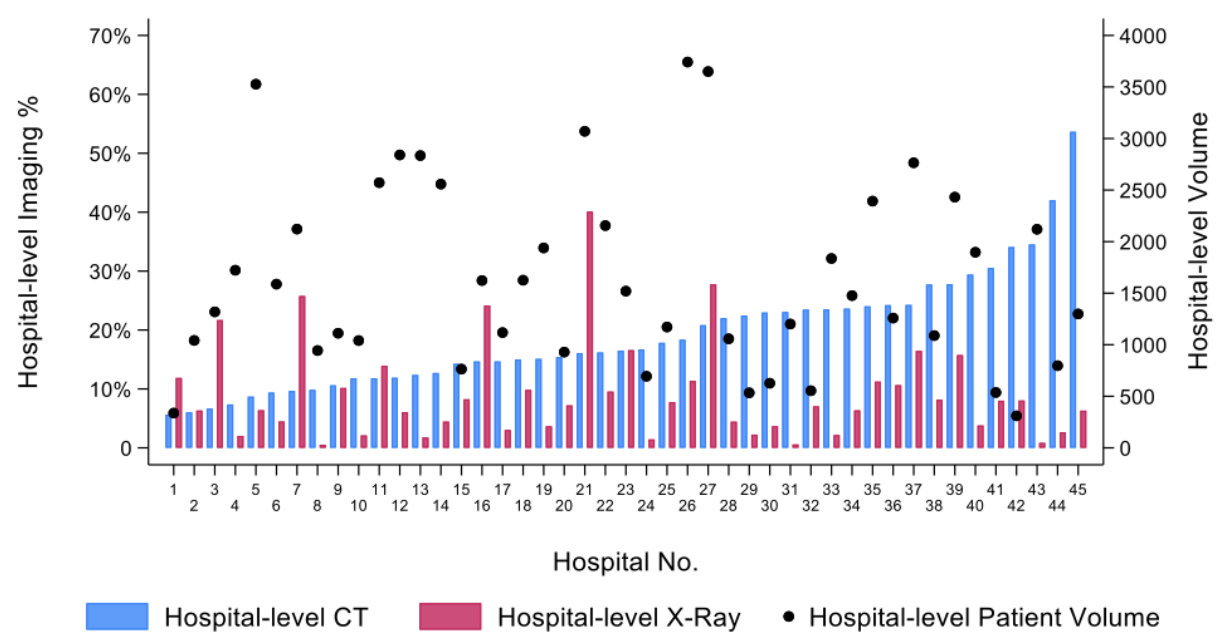
Background: Nasal bone fractures are one of the most common pediatric facial fractures. In the absence of septal hematoma or persistent epistaxis, imaging is not routinely required to confirm the diagnosis. Objective: To determine the rate and variation in use of imaging for the evaluation of nasal injury and assess patient-level factors associated with imaging utilization in pediatric emergency departments (EDs). Design/Methods: We conducted a multi-center, cross-sectional study of children aged 0 to 18 years presenting to a hospital participating in the Pediatric Health Information System (PHIS). We included children with an ICD-10 diagnosis code for nasal injury. We assessed the mechanism of injury and use of diagnostic imaging (x-ray, computed tomography (CT)). We tested the hospital-level association between x-ray and CT utilization and patient volume with Pearson correlations. To determine patient-level predictors of imaging, we estimated logistic regression models with any imaging as the dependent variable and demographic, diagnosis (nasal injury versus nasal fracture), and PHIS-based clinical measures (mechanism of injury, injury severity score) as the independent variables. Results: A total of 73,751 ED visits for nasal injury were analyzed, of which 18,918 ED visits (25.7%) had a diagnosis of nasal fracture (Table 1). Of the 28.8% that underwent imaging, 13,473 (18.3%) had a CT and 7,746 (10.5%) had an x-ray performed. Falls were the most common mechanism of injury (27.1%). Among patients presenting with a nasal injury, age >3 years, census region in the South, a nasal fracture diagnosis, and severe traumatic injury were associated with higher imaging utilization while Black race was associated with lower imaging utilization (Table 2). Imaging utilization varied across hospitals, with hospital-level CT and x-ray utilization ranging from 5.6%-53.7% and 0.5%-40.1%, respectively (Figure 1). As hospital-level patient volume increased, x-ray utilization increased (r=0.33, p< 0.01). CT utilization was not associated with patient volume (r=-0.090, p=0.40) or x-ray utilization (r=-0.04, p=0.70).
Conclusion(s): There is wide variation in the use of diagnostic imaging across US children's hospital EDs. Future guidelines are needed to help standardize imaging use in the management of pediatric nasal injury.
Table 1: Demographic and clinical characteristics of children presenting to the emergency department with nasal injury, stratified by imaging utilization (CT and/or x-ray)
Table 2. Demographic and clinical predictors of imaging utilization (CT and/or x-ray) among children presenting to the emergency department with nasal injury
Figure 1. Variability in hospital-level CT and x-ray utilization among children treated in the emergency department for nasal injury.

 photo")