177 - All in Your HEADSSS: An Epic Approach to Assessing Adolescents
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3170.177
Tiffany Le, University of Florida College of Medicine, Jacksonville, FL, United States; Mariana Diaz, University of Florida Jacksonville, Jacksonville, FL, United States; Taylor Smith, University of Florida College of Medicine, Orange Park, FL, United States; Lisa Awe, University of Florida - Jacksonville, Jacksonville, FL, United States
Resident Physician University of Florida College of Medicine - Jacksonville Jacksonville, Florida, United States
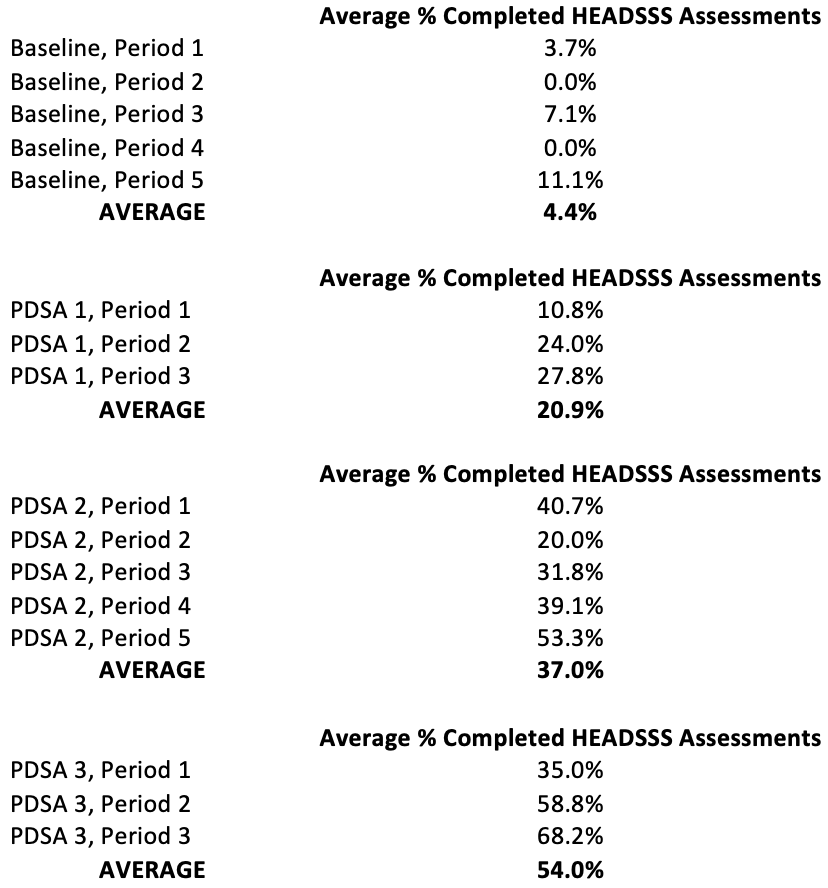
Background: The HEADSSS assessment (Home, Education, Activities, Drugs, Sex/Safety/Suicidality) is a validated tool used to screen for psychosocial risk factors in adolescents. Despite recommendation by the American Academy of Pediatrics, most healthcare encounters do not include a HEADSSS assessment. Barriers as reported by pediatric residents include "it's too busy overnight," "it's awkward to ask family to leave the room," and "I forgot." Objective: We completed this quality improvement (QI) project at a medium-sized children's hospital. According to baseline data, fewer than 10% of adolescents admitted to the hospital's pediatric service had a HEADSSS assessment completed on admission. We endeavored to improve the screening of inpatient adolescents by increasing the HEADSSS Assessment completion rate in adolescents age 12-18 by 25% within nine months of initiation of the first Plan-Do-Study-Act (PDSA) cycle. Design/Methods: We conducted a survey to determine HEADSSS exam barriers; 94% of pediatric residents completed the survey with the most common reason being, "I forgot." Considering this, our main goals were to make the process of completing a HEADSSS assessment easier as well as provide reminders to the residents to complete it. Our baseline data showed < 5% of H&Ps had a completed HEADSSS exam. Patients were excluded if 1) an advanced practice provider completed the admission, 2) they were admitted to a subspecialty service, 3) mental status was altered, or 4) they had a significant intellectual disability. During our first PDSA cycle, we used an Electronic Medical Record (EMR) approach by creating a standardized H&P template that included a section for the HEADSSS assessment with a drop-down box of common questions and answers. Our second intervention was replacing the drop-down boxes with the EMR wildcard symbol, which forced a response from the author prior to signing the note. Our third intervention was creating and placing visual reminders to complete the HEADSSS assessments in resident workrooms. Results: After one PDSA cycle, the percentage of HEADSSS assessments being completed on inpatient adolescent admissions increased by 375% and final results increased 1127% above baseline.
Conclusion(s): Our interventions successfully increased the percentage of completed HEADSSS assessments for adolescents during admission. Future efforts will focus on improving our efforts, expanding to obtain HEADSS exam anytime during admission, as well as determining if screening identifies previously missed opportunities for intervention, such as identifying mental health problems in a patient admitted for unrelated issues.
Average Percentage of HEADSSS Assessments Completed at the Time of Hospitalist Pediatrics Service Admission
Percentage of HEADSSS Assessments Completed at the Time of Hospitalist Pediatrics Service Admission
Table of Each Data Collection Period and the Average Percentage of Completed HEADSSS Assessments

 photo")
.png)
.png)