164 - Decreasing Testing of Febrile Newborns in the Pediatric Urgent Care Prior to Transfer to the Emergency Department
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3158.164
Jerry M. Stultz, Nationwide Children's Hospital, Columbus, OH, United States; Kathleen Sugrue, Ohio State University College of Medicine, Hilliard, OH, United States; Courtney Kirby, Nationwide Children's Hospital, Grove City, OH, United States; cynthia zimm, Nationwide Children's Hospital, Columbus, OH, United States; Luciana Berg, Nationwide Children's Hospital, Columbus, OH, United States
Co-Director Quality Improvement, Division of Urgent Care Nationwide Children's Hospital Columbus, Ohio, United States
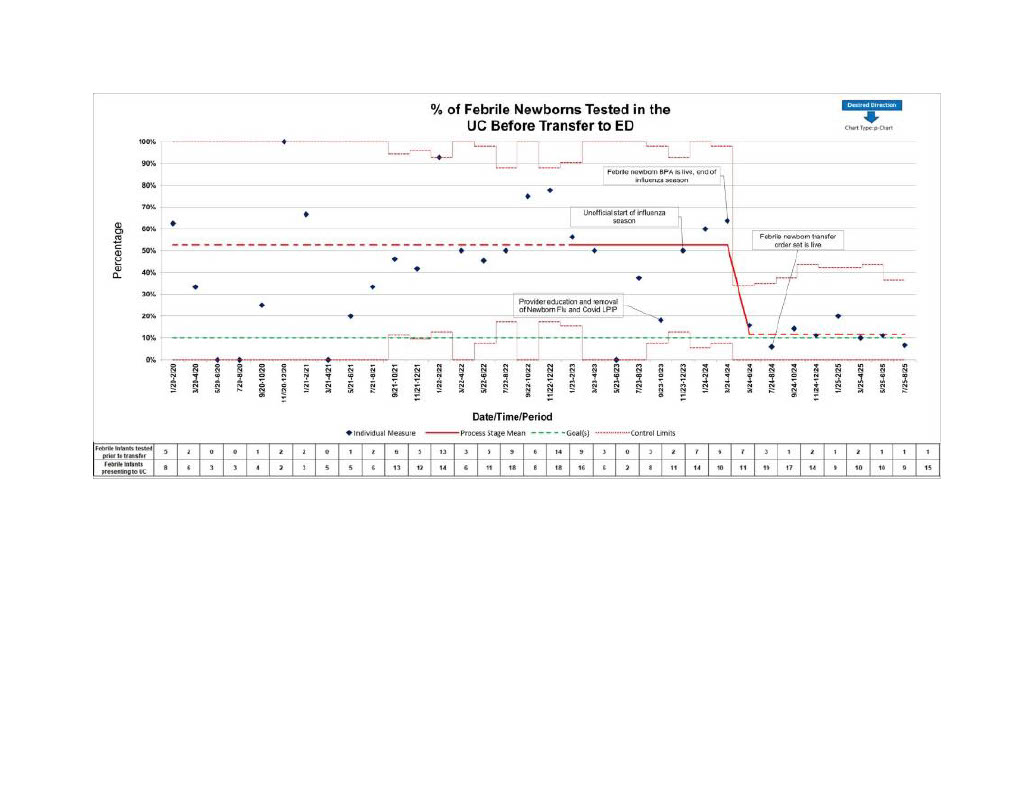
Background: Febrile newborns (FN) presenting to Urgent Care (UC) require a prompt and focused assessment. Nationwide Children's Hospital (NCH) has developed clinical pathways based on American Academy of Pediatrics (AAP) guidelines outlining appropriate age-based evaluations for febrile patients in the first 60 days of life. Offsite UC centers cannot perform all guideline testing in real time; therefore, patients undergo a partial work-up in the UC and are transferred to the emergency department (ED) for the rest of assessment. This is inefficient, delays management, and is not in the best interest of the patient or family. Objective: This quality improvement project focuses on deferring the work-up on febrile newborns in the UC and instead transferring them immediately to the ED. Rapid transfer benefits the patient and family by avoiding repetitive testing and expediting their evaluation and care while reducing the patient's time spent in the UC. Design/Methods: Quality improvement methodology was applied to decrease the percentage of UC febrile newborns tested in the UC then transferred to the ED. A baseline percentage of febrile newborns seen in urgent care who were tested prior to transfer was determined. Multiple interventions, including provider education, EMR best practice advisories (BPA), and an improved workflow were implemented over the first year of the project. Patient data were gathered in 2-month intervals from May 2023 to August 2025 and percentages were plotted on a P-chart. Results: The percentage of febrile newborns tested in the UC prior to ED transfer was established as 53%; the AIM was set at 10% (34% reduction). Post interventions, pretransfer percentages consistently dropped below the control line resulting in a shift of the control line to 10%, thus meeting the project AIM.
Conclusion(s): Some interventions were less effective than others. Educating providers and limiting triage ordered testing based on age were initially successful. However, Covid-19 and influenza testing were frequently ordered in the UC even though these were not indicated. More effective initiatives included implementing a UC-specific BPA that emphasized no tests in the UC, and the creation of a febrile newborn transfer discharge set. The 2024 influenza season saw less Covid-19 and flu testing of these patients in the UC suggesting that the BPA was working. Further planned interventions include a specific EMR note template and discussions with community physicians about sending febrile newborns to the ED instead of the UC.
Percentage of Febrile Newborns Tested in the UC Before Transfer to the ED

 Credit")