Session: Developmental and Behavioral Pediatrics 4: Potpourri
211 - Providing Culturally Effective Care: Pediatric Providers’ Anticipatory Guidance and Developmental Surveillance for Dual-Language Learners
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3203.211
Milton Guendica, Northwestern University, Lincolnwood, IL, United States; Yu Chen, New York University Grossman School of Medicine, New York, NY, United States; Caitlin F. Canfield, NYU Grossman School of Medicine, New York, NY, United States; Anna Miller-Fitzwater, Wake Forest University School of Medicine, Winston-Salem, NC, United States; Mariana Glusman, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States; Adriana Weisleder, Northwestern University, Evanston, IL, United States
PhD Student Northwestern University Lincolnwood, Illinois, United States
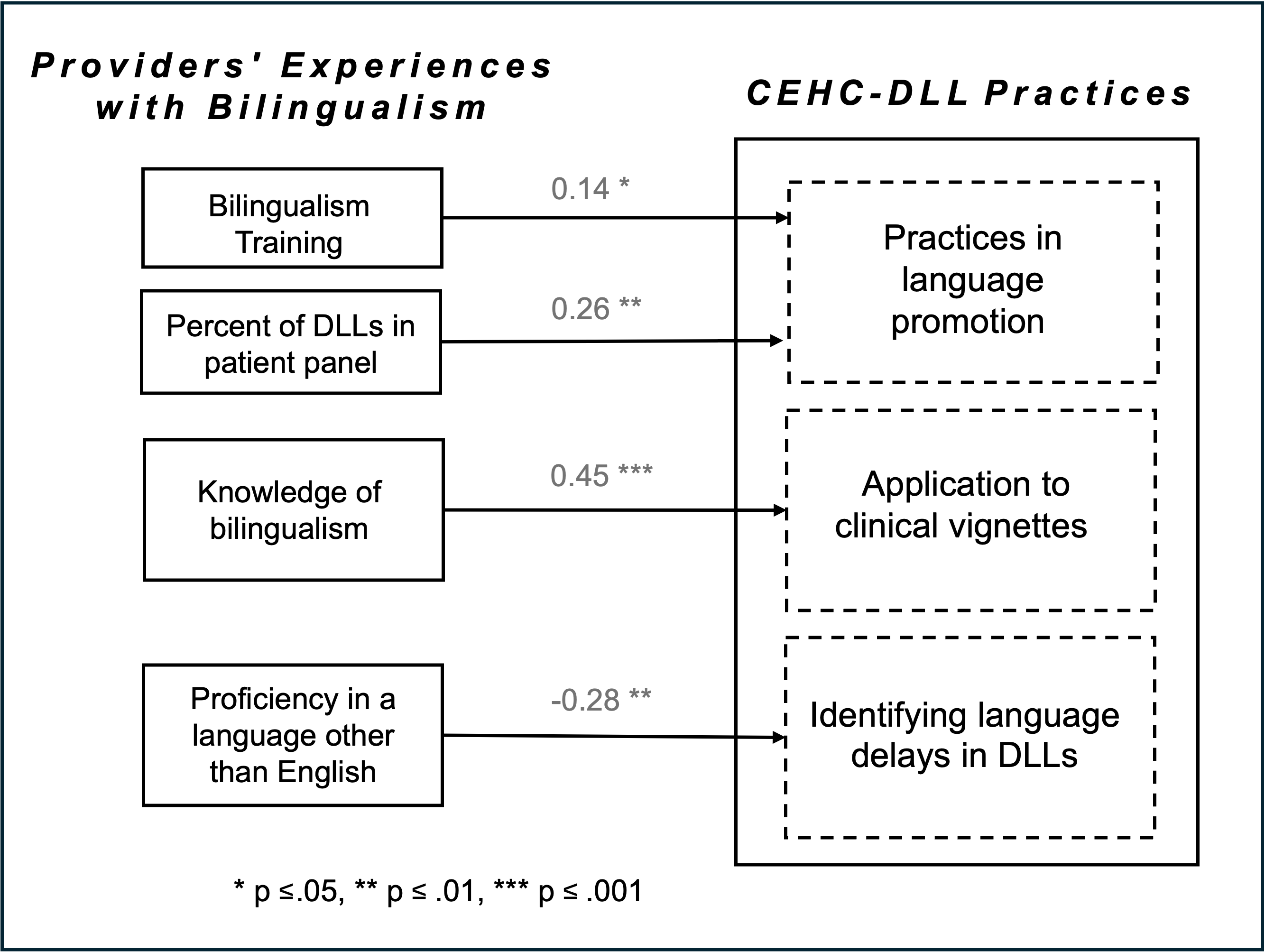
Background: A quarter of all US children are dual-language learners (DLLs). DLLs experience health and academic disparities, including being over/under-identified with language delays and having lower language scores at school entry. Pediatric providers can address these disparities by providing anticipatory guidance on language development and developmental surveillance in ways that are culturally-linguistically responsive. However, little is known about the extent to which providers are prepared to provide culturally effective healthcare for DLLs (CEHC-DLLs) and the factors that influence these practices. Objective: The objectives of this study were to 1) characterize providers' knowledge of bilingualism and their CEHC-DLL practices and 2) determine whether providers' experience with and knowledge of bilingualism are related to their CEHC-DLL practices. Design/Methods: Providers who conduct well-child visits ages 0-5 completed a one-time online survey (N=349; Table 1). Predictors: Experiences with bilingualism: 1) Proficiency in a language other than English (levels 0-3), 2) Bilingualism training (yes-no), 3) Percent of DLL patients (low-high), 4) Knowledge of bilingualism score (based on agreement with 10 evidence-based statements). Outcomes. 1) Self-reported language promotion practices (score based on 6 items), 2) Self-reported difficulty identifying language delays (levels 1-4), and 3) Correct responses to 4 multiple choice clinical vignettes (sum score). Three multiple regressions estimated the independent effects of all predictors on each outcome. Results: Most providers (75%) said they provide anticipatory guidance about bilingual language development, and 79% found it difficult to identify language delays in DLLs. In vignette responses, less than 50% of providers encouraged families of DLLs to use their home language and only 28% effectively identified a language delay. Multiple regressions (Figure 1) indicated that bilingualism training (B=0.14, p=0.04) and a high percentage of DLL patients (B=0.26, p=0.005) were related to greater language promotion practices. Bilingual background was related to providers' reduced difficulty identifying language delays in DLLs (B= -0.28, p=0.002). Finally, knowledge of bilingualism was related to more correct vignette responses (B=0.45, p=0.001).
Conclusion(s): Providers who are bilingual, receive training on bilingualism, and/or frequently encounter DLLs provide more culturally effective health care to DLLs. Results highlight a continued need for bilingual providers as well as training that addresses language development in DLLs.
Table 1. Provider demographics
Figure 1. Links between providers' experiences with bilingualism and their CEHC-DLL practices

 photo")
.png)