Session: Neo-Perinatal Health Care Delivery: Epidemiology/Health Services Research 2
88 - The Virtual Genome Center (VIGOR) study: Implementation of a virtual delivery model for rapid genomic sequencing in safety-net Neonatal Intensive Care Units
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3084.88
Alissa D'Gama, Boston Children's Hospital, Dedham, MA, United States; Sonia Hills, Boston Children's Hospital, Boston, MA, United States; Jessica L. Douglas, Boston Children's Hospital, Boston, MA, United States; Meghan Werner, Boston Children's Hospital, Woburn, MA, United States; Monica Wojcik, Boston Children's Hospital, Boston, MA, United States; Casie A. Genetti, Boston Children's Hospital, Boston, MA, United States; Vanessa j. Young, Boston Children's Hospital, Boston, MA, United States; Timothy Yu, Harvard Medical School, Boston, MA, United States; Pankaj Agrawal, Holtz Children's Hospital Jackson Memorial Hospital, Miami, FL, United States; Margaret Parker, UMass Chan School of Medicine, Worcester, MA, United States
Assistant Professor Boston Children's Hospital Dedham, Massachusetts, United States
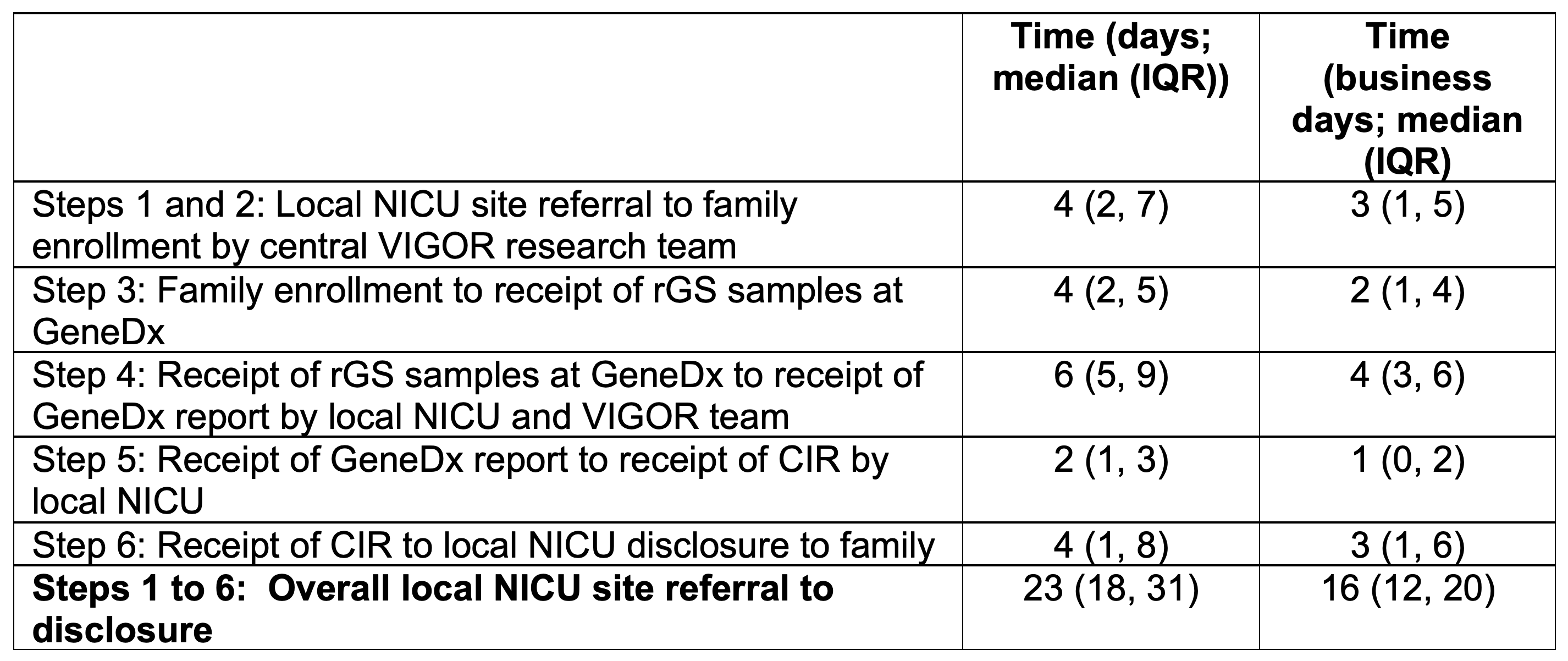
Background: Rapid genomic sequencing (rGS) has high diagnostic and clinical utility in Neonatal Intensive Care Units (NICUs). However, safety-net NICUs that disproportionately serve marginalized populations often lack access to rGS, leading to inequitable outcomes. The Virtual Genome Center (VIGOR) is an innovative virtual delivery model for rGS in safety-net NICUs. Objective: To examine 1) "VIGOR penetration rate" (fraction of enrolled infants who received rGS, had a customized clinical interpretive report (CIR) delivered to the NICU team within 3 business days of the Clinical Laboratory Improvement Amendment (CLIA) vendor report, and had results disclosed to the family); 2) Differences in penetration according to the infant's race/ethnicity and family's preferred language; 3) Timeliness of results reporting and disclosures. Design/Methods: A virtual genome center based at a quaternary referral center remotely supports the rGS process at 10 safety-net NICUs (defined as serving >40% of patients that identify as non-Hispanic black or Hispanic) across 5 states lacking routine access to rGS. This occurs by: 1) Local NICU providers identify eligible infants (Table 1) and refer to the central VIGOR team; 2) The VIGOR team consents and enrolls infants; 3) rGS is sent (infant and up to 2 biological parents); 4) The CLIA vendor (GeneDx) provides a vendor report of results to the local sites and VIGOR team; 5) the VIGOR team creates customized CIRs that are returned to local sites within 3 business days of the vendor report; and 6) Local sites disclose results using CIRs if desired. We measured the overall "VIGOR penetration rate," which was the fraction of enrolled cases who completed all the steps, and differences in penetration according to parent-reported infant race/ethnicity and family's preferred language. We analyzed the median time to completion of the participation flow steps across our study. Results: From 10/2022-9/2025, 199/270 (74%) eligible infants consented and enrolled. Of the 199 enrolled, 185 (93%) completed the study steps. We did not find differences in VIGOR penetration rate according to family's preferred language (English 91% vs Spanish 100%; p = 0.06) or infant race/ethnicity (non-Hispanic white 93% vs other racial/ethnic groups 93%; p =0.85). The time spent on each VIGOR study step is shown in Table 2 stratified by any days and business days. rGS identified genetic diagnoses for 41/192 infants, for a diagnostic yield of 21%.
Conclusion(s): Using a virtual model of supporting safety-net NICUs across the US, we were able to rapidly provide useful genomic sequencing results for families and clinicians.

.png)