120 - Reduction of prolonged antibiotics in culture-negative sepsis (CNS), through a continuous quality improvement (QI) program in the NICU of Hospital Cayetano Heredia (HCH), Lima, Peru.
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3114.120
Juan M.. Graus, Hospital Cayetano Heredia, Lima, Lima, Peru; Naínma M.. Fernández, Hospital Cayetano Heredia, Lima, Lima, Peru; Jaime A.. Zegarra, Universidad Peruana Cayetano Heredia, Lima76, Lima, Peru; Alfonso F. Pantoja, Colorado Permanente Medical Group, Denver, CO, United States; Raul J.. LLanos, Clinica San Felipe, San Borja, Lima, Peru
Attending Neonatologist Hospital Cayetano Heredia Lima, Lima, Peru
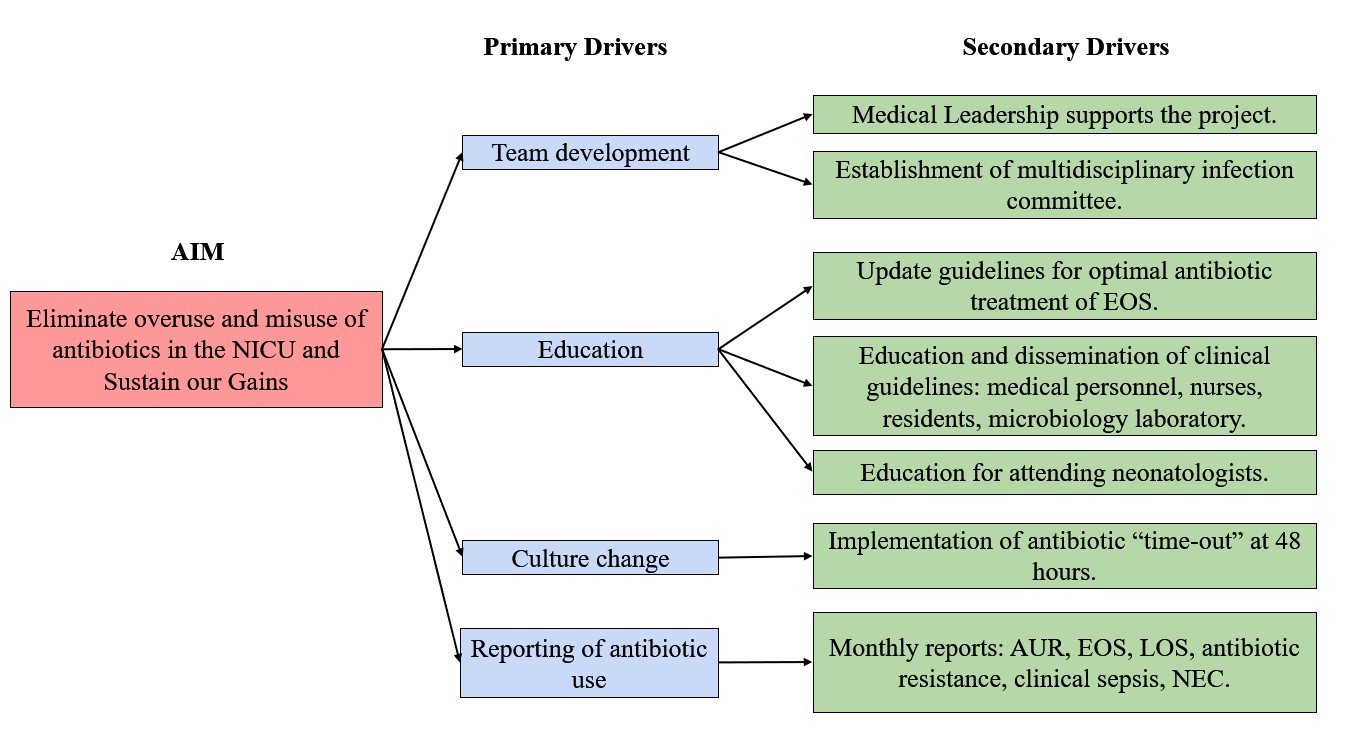
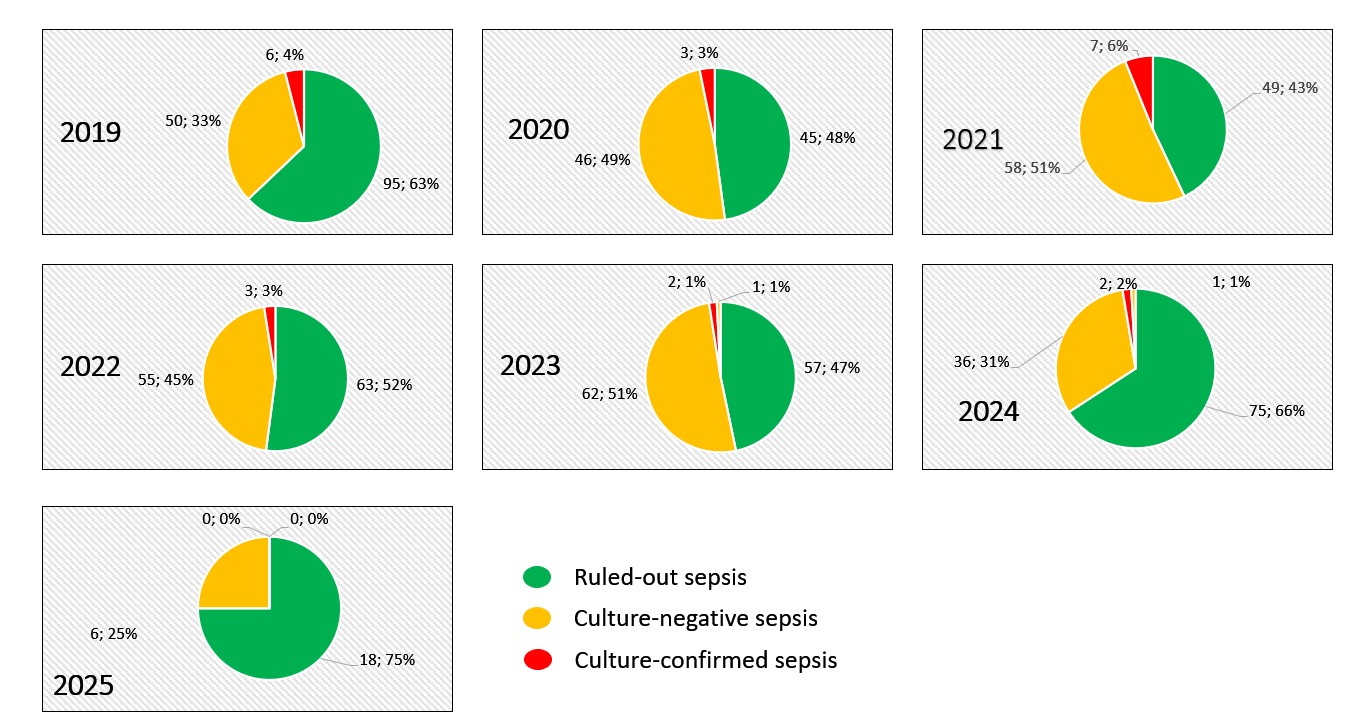
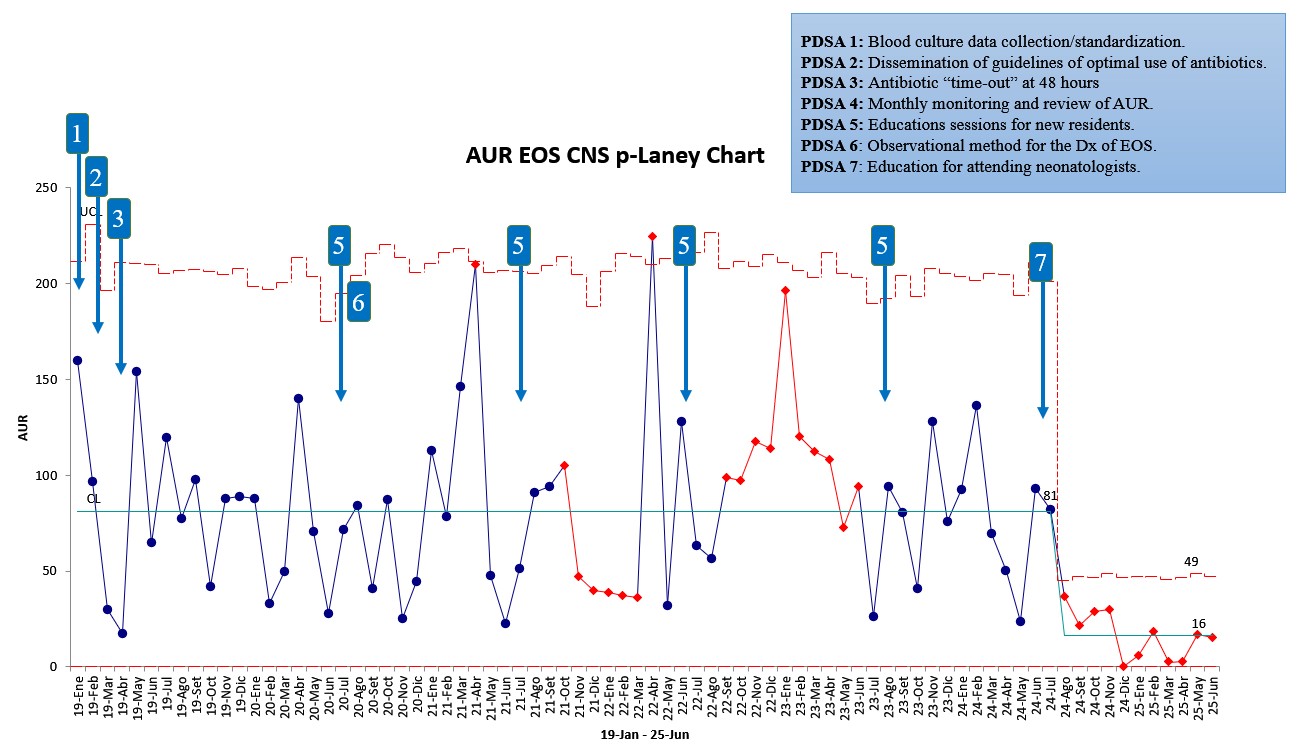
Background: Early-onset sepsis (EOS) presents with nonspecific symptoms and may be confused with normal physiological adaptations in newborns, often leading to the initiation of empirical antibiotic treatment. The rate of culture-positive EOS is less than 1 per 1000 live births; however, infants admitted to NICUs often receive high levels of antibiotic exposure. In 2019, our NICU adopted a protocol to stop antibiotics after 48 hours if the newborn shows clinical improvement and the blood culture remains negative. Despite this, neonatologists still worry about stopping antibiotics too early, and the diagnosis of culture-negative sepsis (CNS) or' Clinical Sepsis" is frequently used to justify continuing antibiotics. Objective: To describe the impact of a continuous QI program on reducing antibiotic use in CNS over the past 5 years in the HCH NICU (Graph 1). Design/Methods: PDSA cycles were implemented following the improvement model, aiming to enhance antimicrobial management in newborns with CNS. The most recent intervention focused on educating the attending neonatologists to observe clinical signs, reduce dependence on inflammatory markers, and increase confidence in microbiological results. To evaluate changes in antibiotic use, we tracked the monthly Antibiotic Usage Rate (AUR) with control charts. AUR represents the total days babies were on antibiotics divided by 1000 patient days. Results: During the study period, we observed a gradual increase in CNS episodes from 2019 to 2023, followed by a substantial decline in 2024 and 2025 (Graph 2). The AUR of EOS shows a 59% decrease over the past year. This change was mainly due to an 80% reduction in antibiotic use in CNS (Graph 3). These shifts are linked to an initiative to educate attending neonatologists, which has led to improved antibiotic utilization. The LOS CNS shows a 44% decrease in antibiotic use over the past year; this change is significant, even though the interventions mainly targeted EOS. We did not see an increase in neonatal mortality in our NICU. This supports the safety of the antibiotic stewardship strategies implemented in our NICU.
Conclusion(s): An educational strategy targeting neonatologists based on observation of clinical findings and trust in microbiological results enhances their confidence in discontinuing antibiotics appropriately.

 Credit")
 photo")