705 - Diagnostic Accuracy of Cardiac Point-of-Care Ultrasound in Children with Myocarditis
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3682.705
Katia Genadry, Boston Children's Hospital, boston, MA, United States; ROBERT HOFFMANN, Boston Children's Hospital, Boston, MA, United States; Andrew F. Miller, Boston Children's Hospital, Brookline, MA, United States; Jeffrey T. Neal, Boston Children's Hospital, Boston, MA, United States; Mark Neuman, Harvard Medical School, boston, MA, United States; Cynthia A. Gravel, Boston Children's Hospital, Boston, MA, United States
Assistant in Pediatrics, Division of Emergency Medicine Boston Children's Hospital Boston Children's Hospital boston, Massachusetts, United States
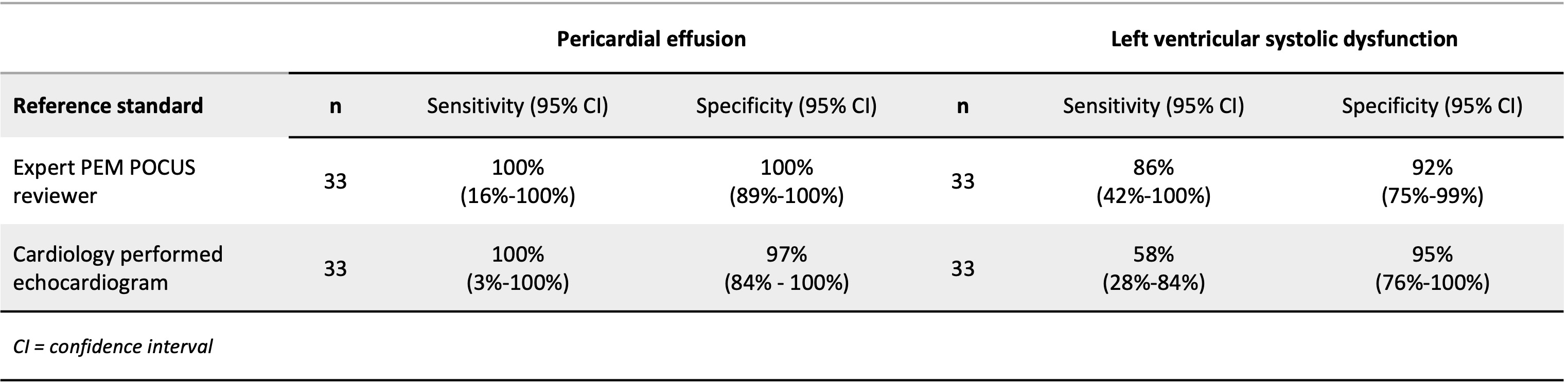
Background: Pediatric myocarditis presents a diagnostic challenge in the emergency department due to its wide range of symptoms and lack of specific early laboratory markers. Cardiac point-of-care ultrasound (POCUS) offers a rapid, radiation-free tool that may help detect key findings such as left ventricular systolic dysfunction and pericardial effusion, but its use in children remains understudied. Objective: This study aims to assess the diagnostic accuracy of cardiac point-of-care ultrasound (POCUS) performed by pediatric emergency medicine (PEM) physicians in children with myocarditis. Design/Methods: This single-center, retrospective study included patients under 21 years of age, without pre-existing cardiac conditions, who presented to a tertiary care emergency department with myocarditis from 2010-2024. Patients were included if they received both cardiac POCUS and a cardiology-performed echocardiogram at the initial visit. Test characteristics for detecting left ventricular (LV) systolic dysfunction and pericardial effusion were calculated using PEM POCUS expert review and echocardiography as reference standards. Results: Thirty-three patients met inclusion criteria. Compared with expert POCUS interpretation, PEM-performed POCUS demonstrated a sensitivity of 86% (95% CI, 42-100) and specificity of 92% (95% CI, 75-99) for LV systolic dysfunction, and a sensitivity of 100% (95% CI, 16-100) and specificity of 100% (95% CI, 89-100) for pericardial effusion. Compared with echocardiography, PEM POCUS had a sensitivity of 58% (95% CI, 28-84) and specificity of 95% (95% CI, 76-100) for LV systolic dysfunction, and a sensitivity of 100% (95% CI, 3-100) and specificity of 97% (95% CI, 84-100) for pericardial effusion.
Conclusion(s): Cardiac POCUS performed by PEM physicians has excellent accuracy for detecting pericardial effusion and for ruling in significant LV systolic dysfunction in pediatric myocarditis. However, it should be used cautiously to rule out systolic dysfunction, especially in children with mild presentations.
Demographic characteristics of patients
Test characteristics of cardiac POCUS for pericardial effusion and systolic dysfunction in pediatric patients with myocarditis
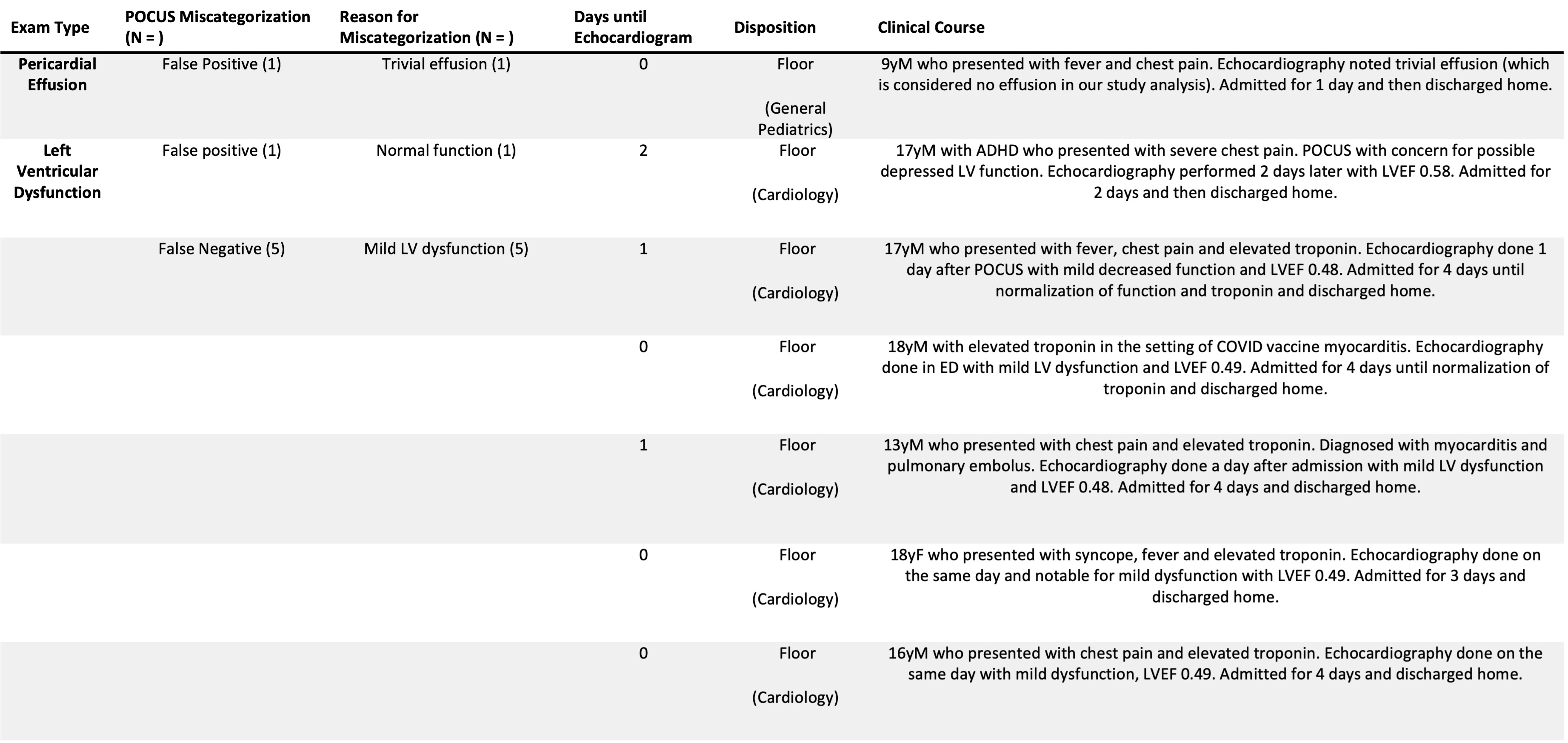
Summary of pediatric myocarditis patients mischaracterized by cardiac POCUS


.jpg)