301 - A US Survey of Clinical Enteral Nutrition Practices in Level 2, 3, and 4 NICUs
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3290.301
Bethany S. Hodges, Mead Johnson Nutrition, St Joseph, MI, United States; Heather V. Evans, Mead Johnson Nutrition, Waunakee, WI, United States; Alayne M. Gatto, Mead Johnson Nutrition, Bloomingdale, GA, United States; Austin Michalski, C.S. Mott Children's Hospital, Chelsea, MI, United States; Lisa M.. Beatrice, Mead Johnson Nutrition, Weymouth, MA, United States; Katina L. Langley, Mead Johnson Nutrition, Goodyear, AZ, United States; Jodee Le Vin, Mead Johnson Nutrition, Chesterfield, MO, United States; Deborah M. Abel, Florida International University, Miami Beach, FL, United States
Medical Science Liaison Mead Johnson Nutrition St Joseph, Michigan, United States
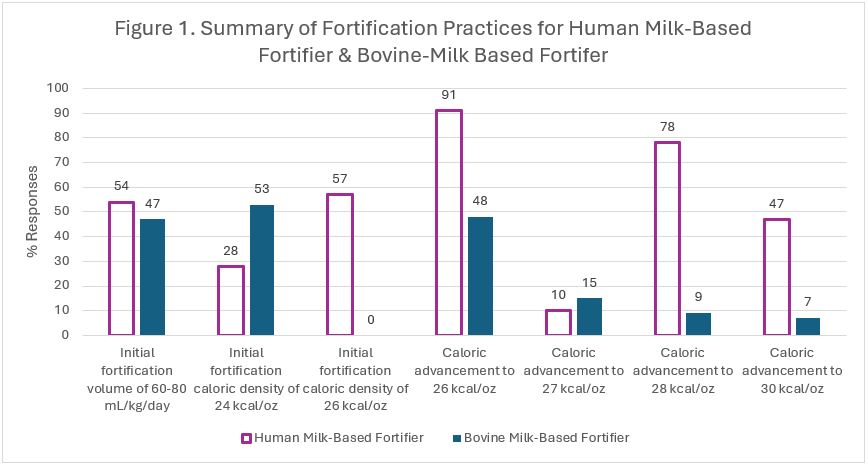
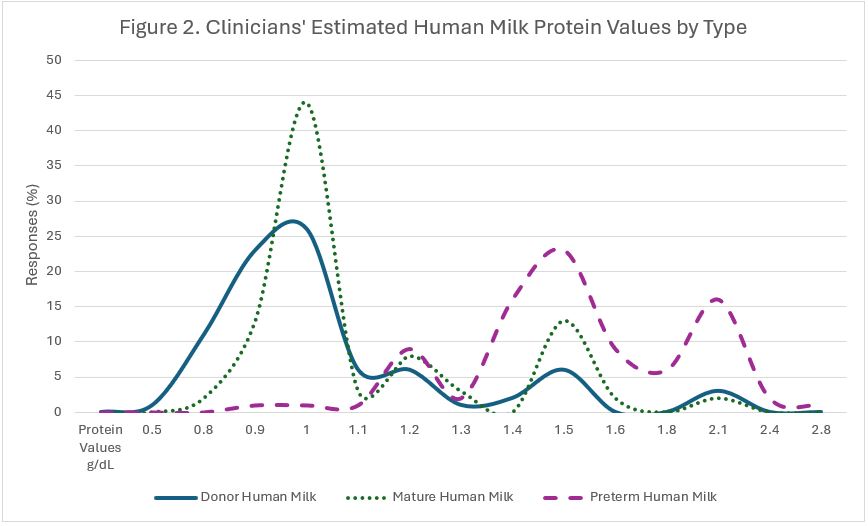
Background: US NICUs lack standardized enteral nutrition practices. This survey describes current practices. Objective: Describe current clinical enteral nutrition practices among healthcare professionals (HCPs) in US NICUs. Design/Methods: An anonymous electronic survey of US HCPs was conducted June-July 2025. Respondents were registered dietitians (RDs), nurse practitioners (NPs), neonatologists, and physician assistants (PAs) working at least 8 hours per month in Level 2, 3, or 4 NICU. Descriptive statistics were used. IRB approval (IRB#MOD02576919) was granted by Advarra (exempt status). A single author secured data. Formal consent was not required; participation was voluntary. Results: A survey of 234 clinicians from 40 US states investigated current enteral nutrition (EN) practices. Respondents included RDs (80.8%), NPs (10.3%), neonatologists (6.84%), and PAs (2.14%) from Level II (4.27%), Level III (52.1%), and Level IV (43.6%) NICUs. Most respondents have standardized feeding (95.9%) and colostrum administration (74.7%) protocols. When mother's milk is unavailable, 44.8% initiate only donor milk, and 51.5% initiate donor milk, preterm formula, and transitional 22 calorie formula. Eligibility criteria for donor milk usage were determined by gestational age (69.7%), while duration was determined by a combination of criteria: gestational age (85.9%), weight (56.2%), clinician discretion (47.6%), and day of life (34.6%). Fortifier preferences were driven by scientific evidence (57.8%) and tolerance (45.5%). Fortifier use included bovine milk-based (BMBF, 49.5%), human milk-based (HMBF, 12.0%), or both (38.0%). Figure 1 illustrates HMBF/BMBF practices. Human milk analyzer use was minimal (8.70%), with cost as the primary barrier. While most clinicians did not use different caloric values for various human milk types, nearly half (48.4%) reported using different protein estimations for donor, mature, or preterm human milk (Figure 2). Table 1 details enteral practices. Key findings include high rates of in-hospital fat, protein, iron, vitamin D, and zinc supplementation. The promotion of HM continues with clinicians reporting 51-75% of infants receiving HM at hospital discharge. Feeding densities vary from 22-30 kcal/oz at hospital discharge, with the most common caloric value at 24 kcal/oz.
Conclusion(s): This survey highlights significant variability and notable trends in US NICU EN practices. These findings highlight the need for further research to establish best practices and develop national, evidence-based guidelines for standardizing care in premature and critically ill infants.
Figure 1. Summary of Fortification Practices for Human Milk-Based Fortifier & Bovine-Milk Based Fortifier
Figure 2. Clinicians' Estimated Human Milk Protein Values by Type


.jpg)
