196 - Derivation of Pediatric Emergency Preparedness Checklist for Urgent Care Centers
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3188.196
Haroon Shaukat, Children's National Health System, Washington, DC, United States; Kamal Abulebda, Riley Hospital for Children at Indiana University Health, Indianapolis, IN, United States; David Mathison, PM PEDIATRICS, Bethesda, MD, United States; Marc Auerbach, Yale School of Medicine, New Haven, CT, United States; Pavan Zaveri, Children's National Health System, Washington, DC, United States; Matthew Yuknis, Indiana University School of Medicine, Indianapolis, IN, United States
Associate Professor of Clinical Pediatrics Indiana University School of Medicine Indianapolis, Indiana, United States
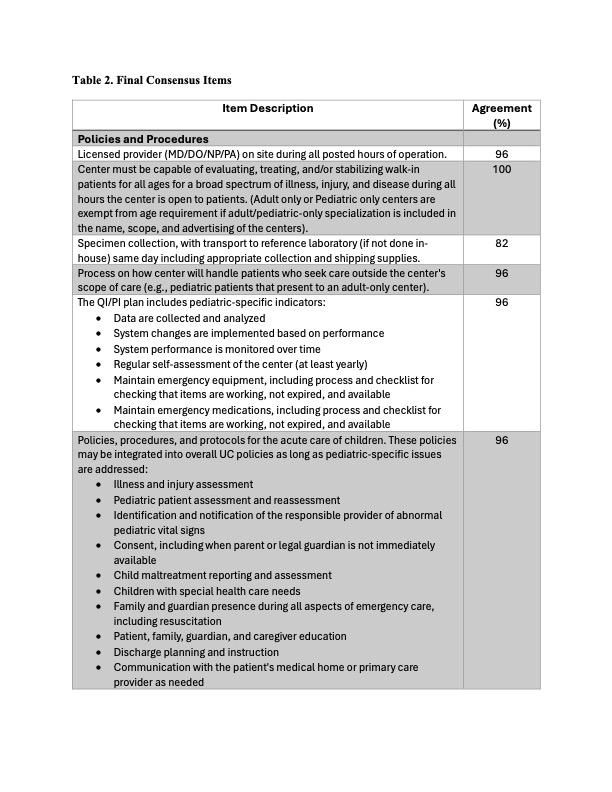
Background: Pediatric readiness/preparedness (coordination, personnel, quality improvement, safety, policies, and equipment) are associated with lower mortality among children with critical illnesses or injuries in emergency departments. However, this has not been evaluated at the urgent care center level. Objective: To develop a consensus-based pediatric emergency preparedness checklist tailored for urgent care centers, addressing policies, procedures, personnel, equipment, and medications necessary to stabilize critically ill or injured children prior to transfer. Design/Methods: A modified Delphi methodology with a purposive sample of 30 nationally recognized physician experts in urgent care medicine, pediatric emergency medicine, or pediatric critical care medicine was conducted. The proposed list derived from urgent care accreditation standards, published pediatric readiness guidelines and literature review, contained 28 comprehensive items, many of which had multiple sub-components totaling 169 individual items. These 28 items spanned across policy/procedures, personnel, equipment, and medications. Consensus was predefined as >80% agreement for inclusion to the next round. Items receiving < 80% agreement were removed from the subsequent round. Respondents evaluated these proposed items until consensus saturation was achieved with an opportunity to provide textual feedback in each round. This was achieved after three iterative rounds (May 2024-July 2025). Results: 22/30 (73%) of invited respondents completed all rounds. In round 1, 26 of 28 items achieved consensus; Round 2 produced consensus on 22 of 26 items; and Round 3 finalized 22 items with 100% consensus. Textual feedback highlighted distinctions between urgent care and emergency departments, deemphasizing items such as advanced airway equipment, an expansive list of non-emergent medications, and disaster preparedness. The final framework included 12 policy/procedure items, 2 personnel items, 7 equipment items, and 1 medication item.
Conclusion(s): Through expert consensus, a pediatric emergency preparedness checklist for urgent care centers was developed. This tool provides actionable guidance for facilities to enhance pediatric readiness while recognizing the resource and scope limitations inherent to urgent care practice. Adoption of this framework can standardize preparedness and improve safety for children experiences emergencies in urgent care settings.

.jpg)