568 - Enhancing Skill Retention and Transfer in Neonatal Intubation Training: A Pilot RCT with Contextual Interference
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3549.568
Jasmine Antoine, The University of Queensland, Brisbane, Queensland, Australia; Kirsty L. McLeod, Clinical Skills Development Service, Brisbane, Queensland, Australia; Peter S. Cunningham, Mater Research, Brisbane, Queensland, Australia; Tamsin Roberts, University of Queensland, Brisbane, Queensland, Australia; Fiona Hutchinson, Mater Mothers Hospital, Brisbane, Brisbane, Queensland, Australia; Richard M. Mausling, Mater Health Services, South Brisbane, Queensland, Australia; Luke A. Jardine, Mater Mothers' Hospital, South Brisbane, Queensland, Australia; Mia L. McLanders, Metro North Health, Herston, Queensland, Australia; Helen G.. Liley, The University of Queensland, South Brisbane, Queensland, Australia
Neonatoologist The University of Queensland Brisbane, Queensland, Australia
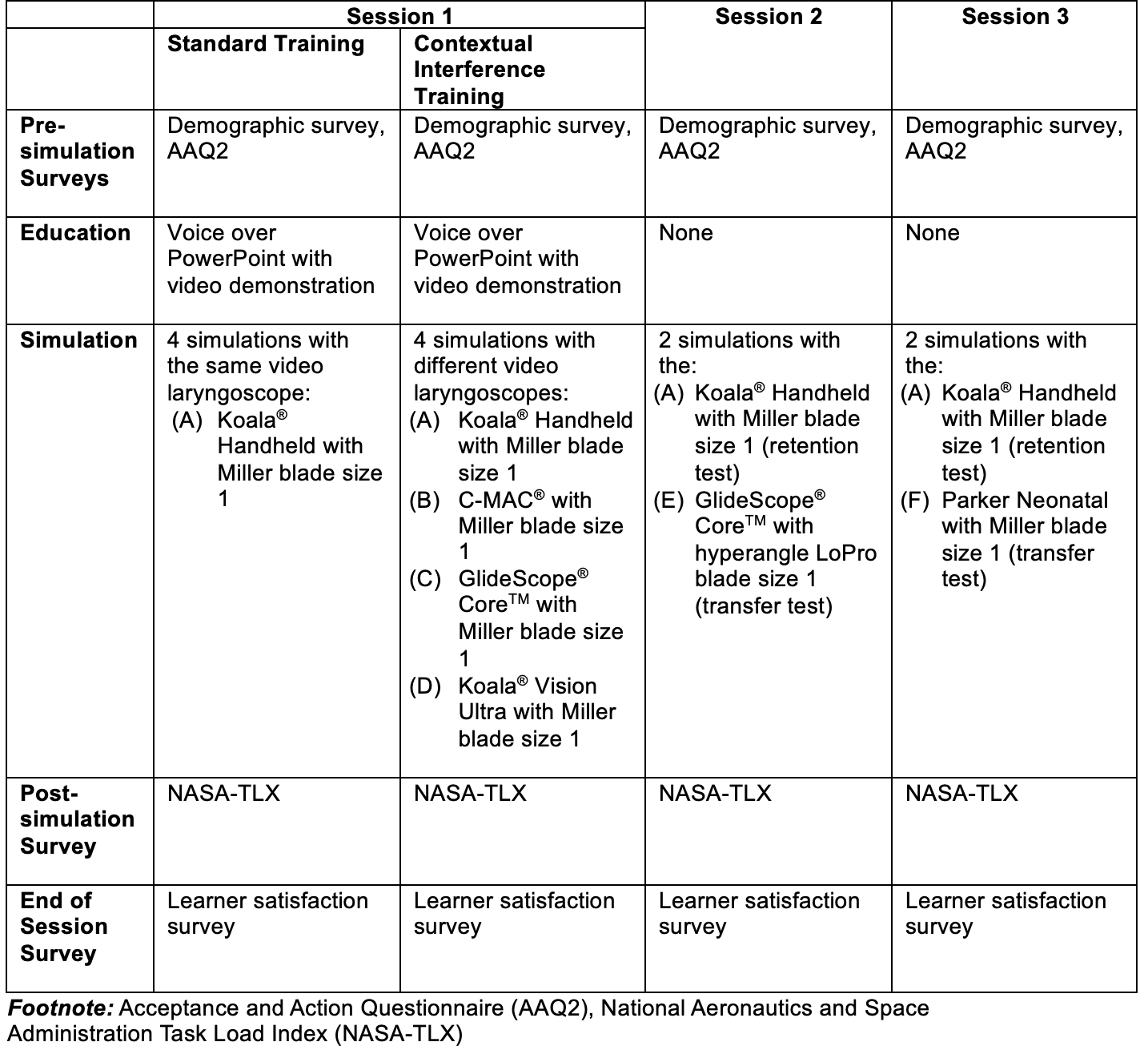
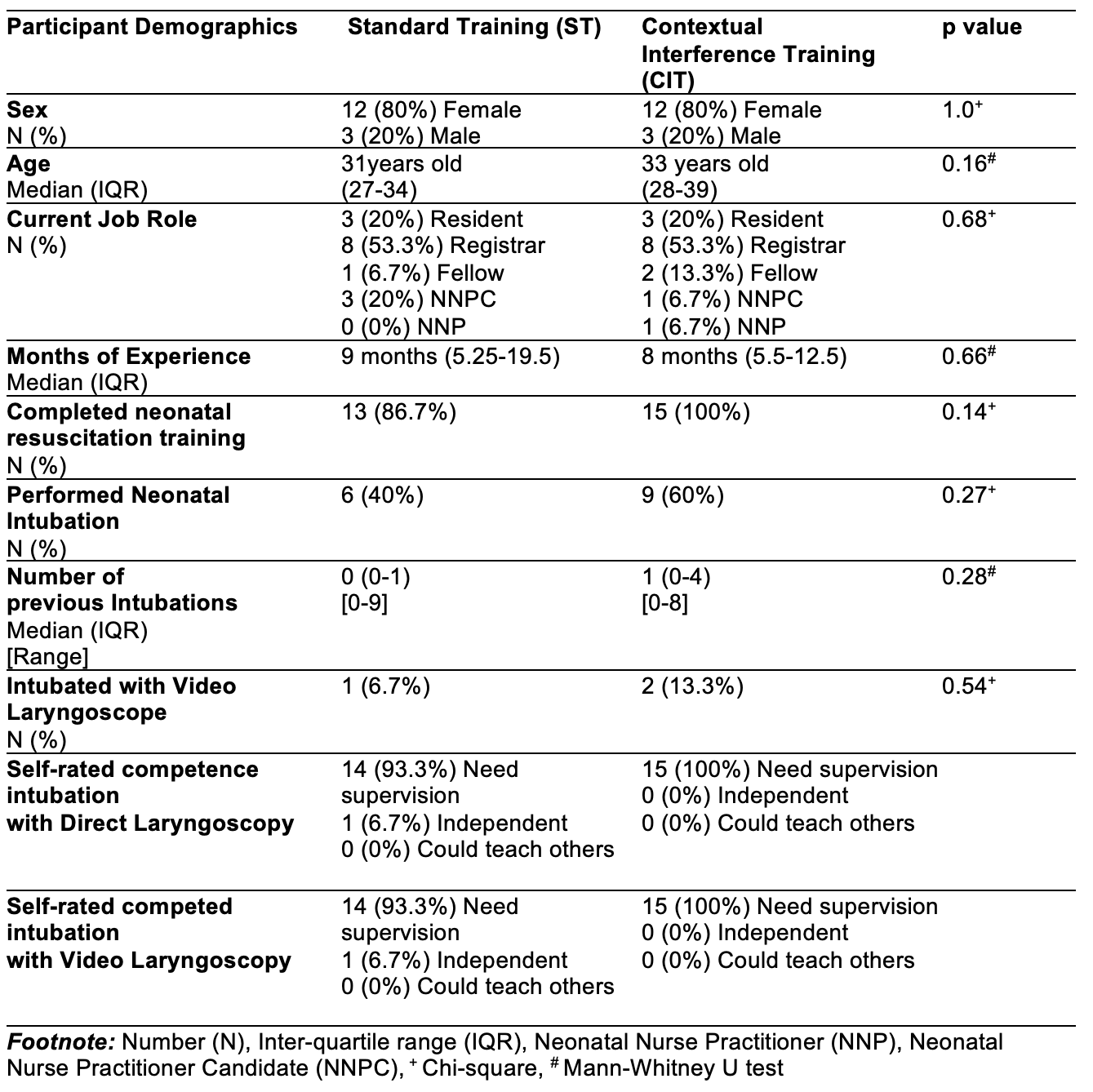
Background: Neonatal intubation training usually focuses on individual technical skill acquisition, often overlooking essential non-technical skills such as team coordination and communication. There is little evidence regarding training approaches to promote skill retention and skill transfer, affording resilience to variations in team composition, clinical environments or equipment. Contextual interference (CI) is a motor learning theory that has been effective in enhancing skill retention and transfer. Objective: To evaluate the feasibility of incorporating CI into neonatal intubation training for novice clinicians and to assess effectiveness for improving skill retention and transfer compared to standard training. Design/Methods: A pilot two-arm simulation study randomized novices ( < 10 intubations) 1:1 to either standard training or CI training. In session both groups received education and completed 4 simulations to assess skill acquisition. The standard training group used the same video laryngoscope (VL), and the CI group used a different VL for each simulation. Session 2 and 3 assessed skill retention with a familiar VL and skill transfer to a novel VL. Outcomes included time to successful intubation, first pass success, overall success, number of attempts, Neonatal Intubation Scoring Instrument (NISI) scores, and non-technical skills. Table 1 outlines the study components. Results: Thirty participants' baseline demographics are shown in Table 2. All participants attended all 3 simulation sessions. Groups differed significantly in psychological flexibility.
Cox regression indicated no significant effect of training type on time to successful intubation (Table 3). Comparing the two groups, the CI training group performed better than the standard training in one measure (overall success). There was no inter-group difference in performance at skill retention or transfer testing of first pass success, number of attempts, and NISI (scored by 2 neonatologists, with good to moderate inter-rater reliability). All participants communicated and responded to the patient's deterioration in all sessions. Learner satisfaction was high for both training groups.
Conclusion(s): This is the first study to apply CI to resuscitation training. Learners tolerated the exposure to novel VLs, with high learner satisfaction and 100% retention rate, confirming feasibility of the training method. CI did not improve skill retention or transfer when compared to standard training, but a larger trial study, stratified for psychological flexibility at baseline may be needed.
Table 1: Pilot Study Components
Table 2: Baseline Participant Demographics
Table 3: Total Time to Successful Intubation and First Pass Success

 photo")
.png)
