318 - Retinopathy of Prematurity and its relationship with Postnatal Weight gain in Premature infants and IUGR infants - Retrospective cohort Study
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3307.318
Hemanthi Durga Veligaram, University of Kentucky College of Medicine, Richmond, KY, United States; Sanchayan Debnath, University of Kentucky College of Medicine, Louisville, KY, United States; Aspen Duncan, UKHC - NICU, Lexington, KY, United States; Alisa B McKinney-Whitlock, University of Kentucky College of Medicine, Lexington, KY, United States; Susan D D. deGraaff, UK Department of Pediatrics, Nicholasville, KY, United States; Hong Huang, University of Kentucky, Lexington, KY, United States
Fellow Physician University of Kentucky College of Medicine Richmond, Kentucky, United States
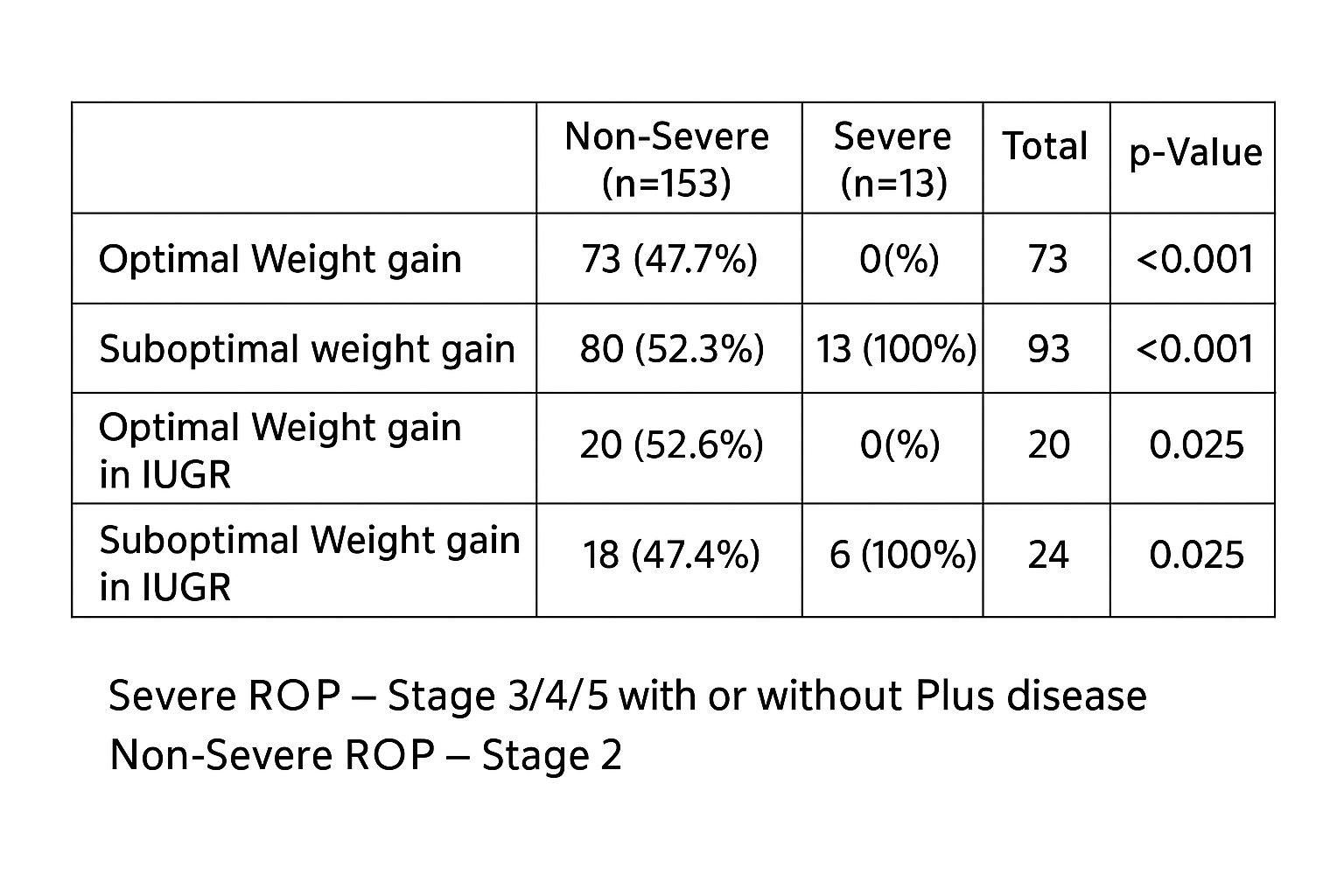
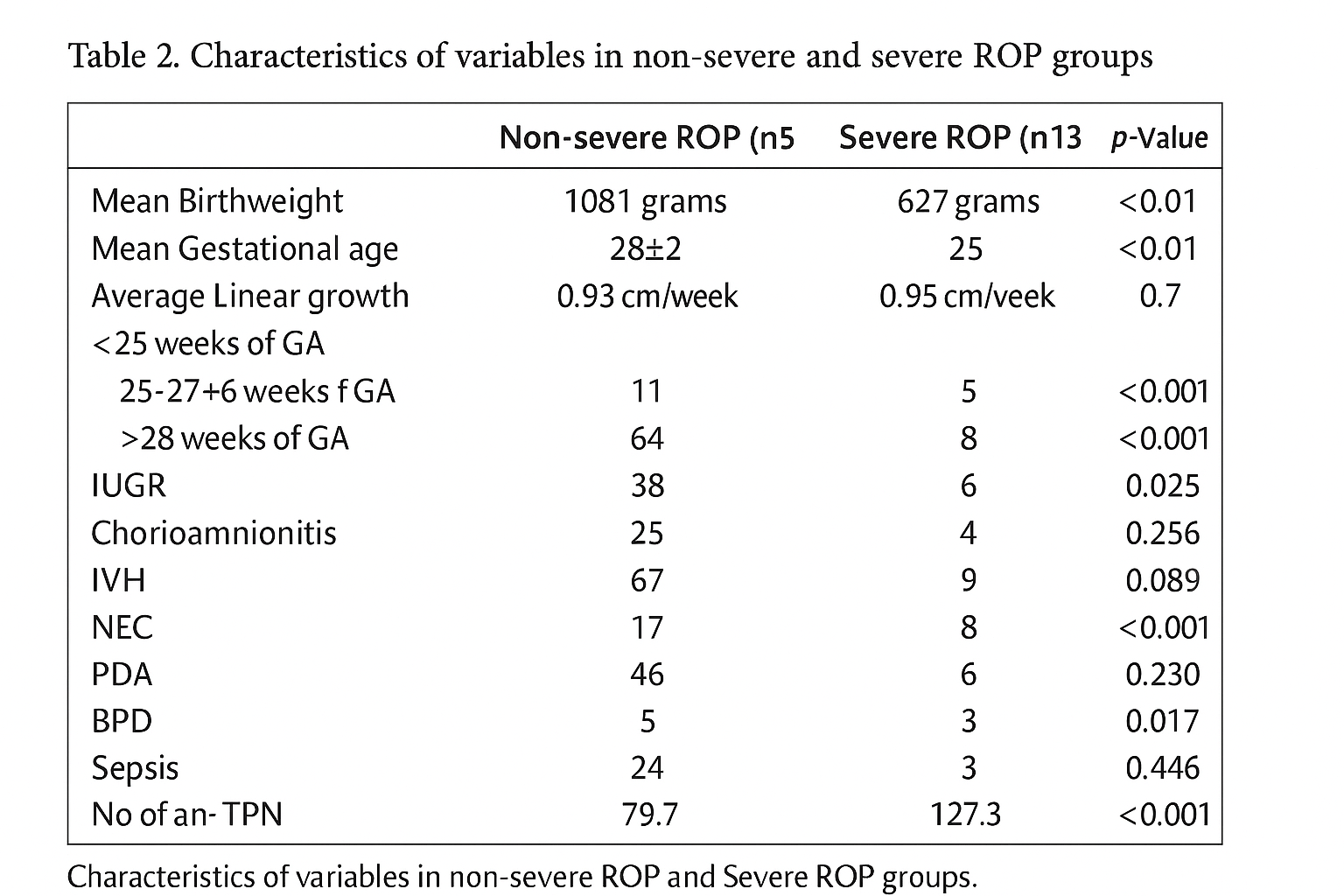
Background: Retinopathy of prematurity (ROP) is a disorder of abnormal retinal vascularization in preterm infants and a leading cause of childhood blindness. With improved survival of extremely preterm infants, ROP incidence has risen. Established risk factors include low gestational age, low birth weight, oxygen exposure, and morbidities such as necrotizing enterocolitis (NEC), sepsis, and intraventricular hemorrhage (IVH). Recent evidence shows poor early postnatal weight gain as a strong predictor for ROP, while adequate growth appears protective. This study examined the relationship between postnatal weight gain and ROP incidence and severity, including its impact in intrauterine growth-restricted (IUGR) infants. Objective: 1. Analyze the relation of postnatal weight gain with the incidence and severity of ROP in level IV NICU 2. Determine whether optimal post-natal weight gain affects the incidence of ROP in IUGR infants Design/Methods: An observational, retrospective cohort study was conducted at the Level IV NICU, Kentucky Children's Hospital, including preterm infants (22-31 weeks' gestational age) who met ROP screening criteria between April 2023 and April 2024. IRB approved the study in November 2024. Infants with congenital anomalies, transfers, or loss to follow-up were excluded. Of 195 charts reviewed, 166 met the inclusion criteria. Data collected included demographics, birth weight, IUGR status, perinatal factors (chorioamnionitis, ventilation, TPN, NPO), weekly weight gain, labs (CRP, albumin), comorbidities (NEC, BPD, IVH, PDA, sepsis), and ROP outcomes (initial, worst, and discharge stage). Results: Mean birth weight was 1,045 g, mean gestational age 28 weeks, and mean weekly weight gain 173 g/kg/week. Thirteen infants (7.8%) developed severe ROP (stage ≥3 ± plus disease). Infants with severe ROP had lower birth weight (627 g vs. 1,081 g; p< 0.01) and GA (25 vs. 28+2 weeks; p< 0.01). Optimal weekly weight gain (105-175 g/kg/week) was achieved in most non-severe cases, while 100% of severe ROP cases had suboptimal gain ( < 105 g/kg/week) (p < 0.01). All treated infants (laser or Avastin) had suboptimal weight gain. Of 44 IUGR infants, mean weight gain was 197.5 g/kg/week; all with suboptimal growth developed severe ROP, whereas none with optimal growth did (p < 0.01).
Conclusion(s): Poor postnatal weight gain is strongly associated with increased risk and severity of ROP. Adequate early growth appears protective, even among IUGR infants, emphasizing the importance of optimized nutrition and growth monitoring in preventing severe ROP.
Data Analysis/Results
Table 2. Characteristics of variables in non-severe and severe ROP