152 - The Development of an Apparent Cause Analysis Program at a Quaternary Care Hospital
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3146.152
Kate E.. Humphrey, Boston Children's Hospital, Boston, MA, United States; Lisa Rickey, Boston Children's Hospital, Boston, MA, United States; Jennifer Treseler, Boston Children's Hospital, West Roxbury, MA, United States; Victoria Renaldi, Boston Children's Hospital, Manchester, NH, United States; David J. Davis, Boston Children's Hospital, Boston, MA, United States; Britta M. Egeland, Boston Children's Hospital, Cambridge, MA, United States; Dorothy M. Miller, Boston Children's Hospital, Boston, MA, United States; Sara Toomey, Boston Children's Hospital, Cambridge, MA, United States
Medical Director for Patient Safety Boston Children's Hospital Boston, Massachusetts, United States
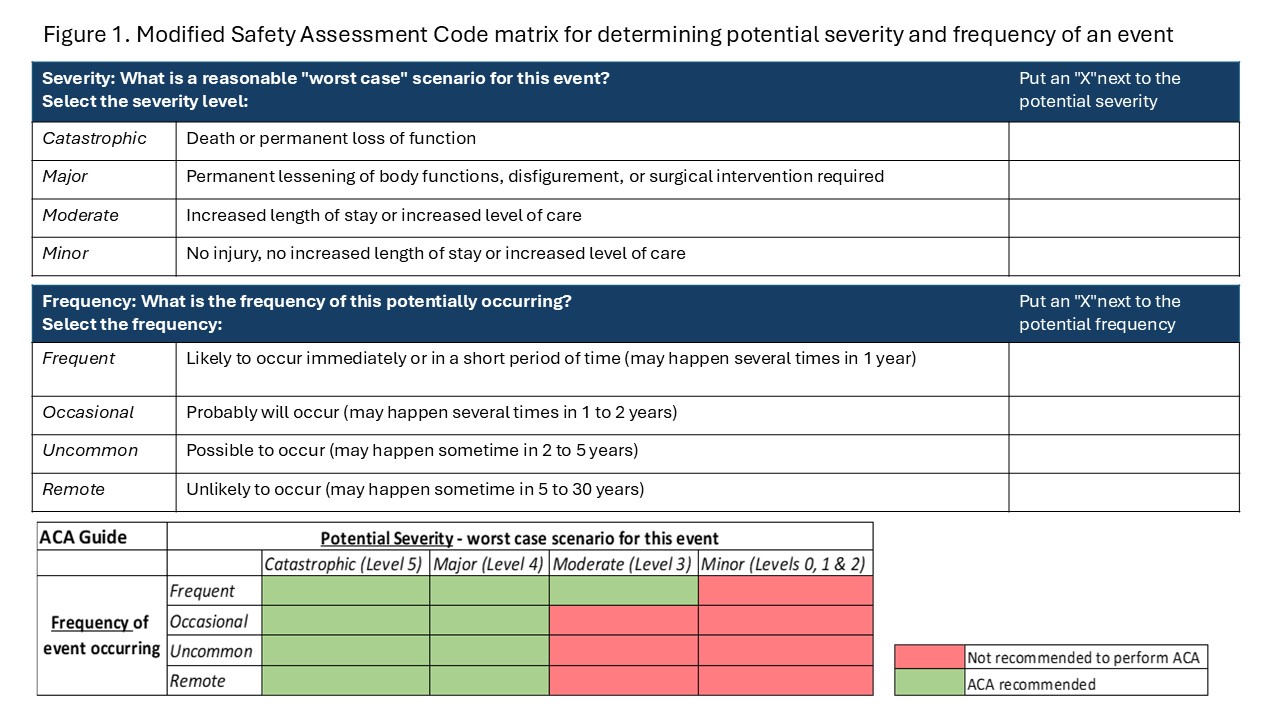
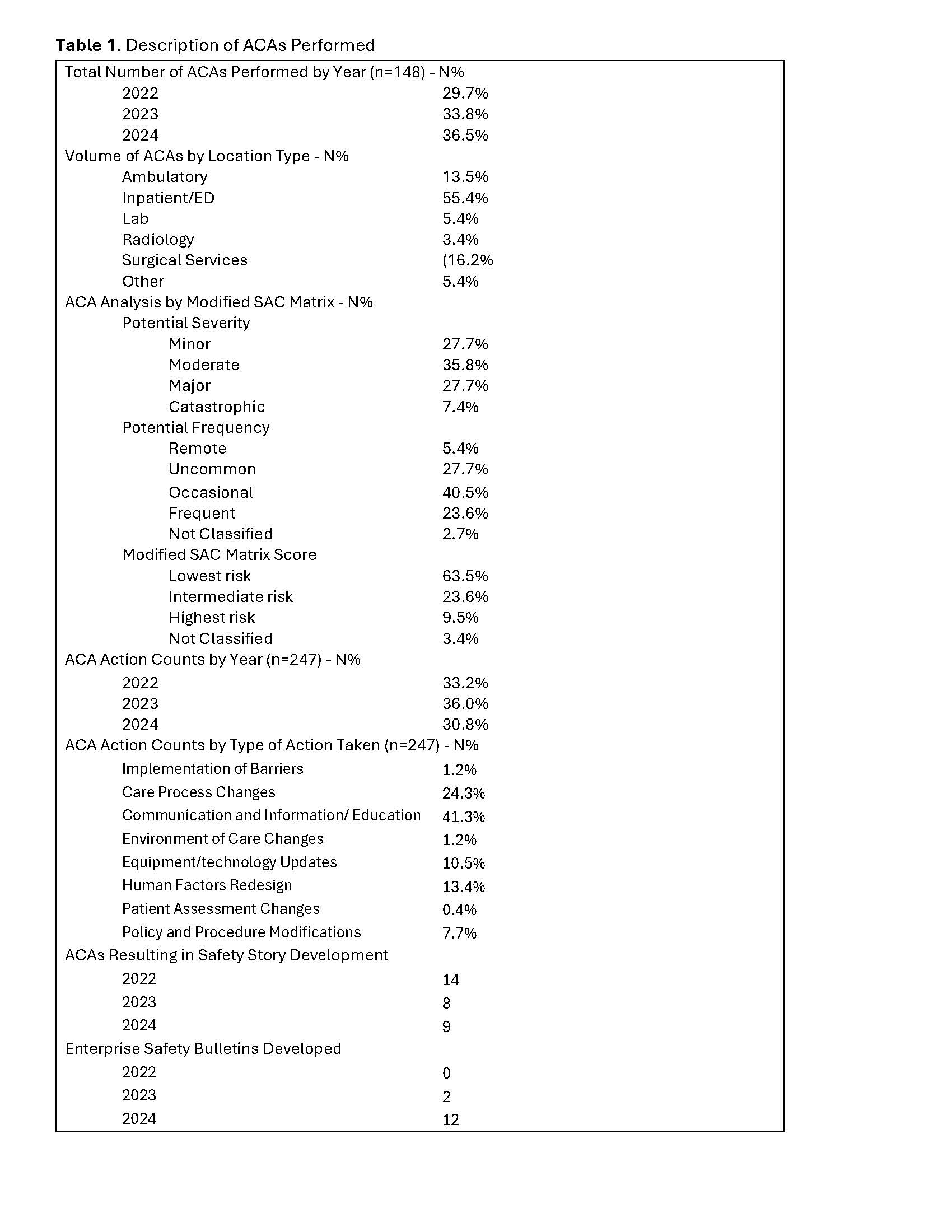
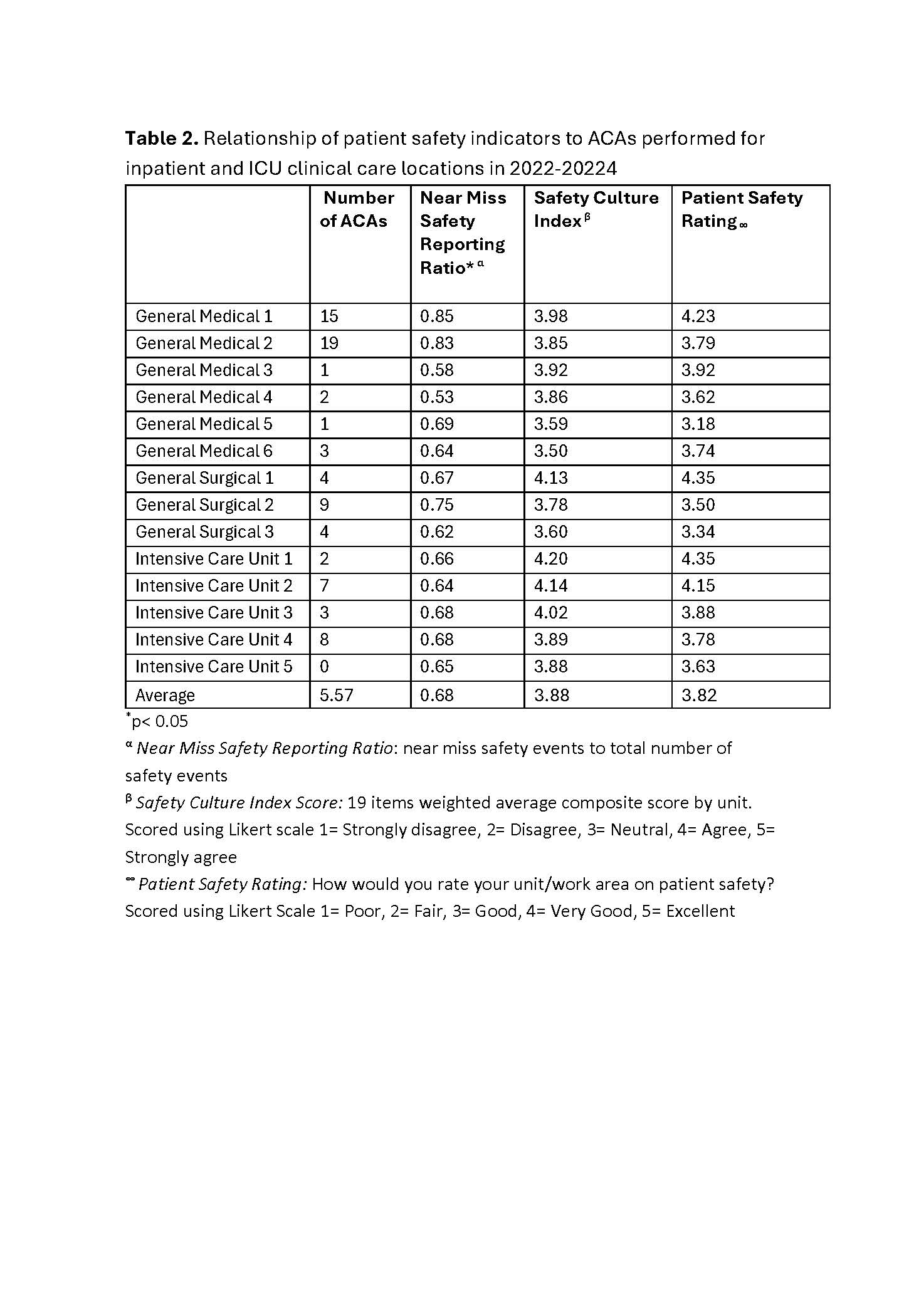
Background: Apparent cause analyses (ACAs) are a structured safety tool for analysis of near-miss and precursor safety events. Led by local safety leaders, these reviews can support safety culture by identifying vulnerabilities, developing action items, and creating shared learnings. We sought to develop an ACA Program at a quaternary care hospital. Objective: To describe an approach to establishing an ACA program and to assess the association of unit-based engagement with performing ACAs with patient safety culture indicators. Design/Methods: We developed an organizational approach to support local review of near-miss and precursor safety events through a reinvigorated ACA Program in 2021. A current state assessment informed process optimization including: (1) standardized initiation criteria with a modified Safety Assessment Code (SAC) matrix using potential severity, frequency and aggregate risk score [Fig.1], (2) centralized analysis with review of actions, and (3) creation of an organizational learnings communication strategy. From 2022-2024, we performed an analysis of ACAs, modified SAC matrix scoring, and crafted safety stories shared more broadly via a monthly Safety Learnings Bulletin. To assess unit-based engagement of ACA performance with patient safety culture indicators, we analyzed ACAs completed by inpatient unit and the Safety Culture Index, Patient Safety Rating Index, and near-miss safety incident ratio. Analyses were conducted using Spearman Rank Correlation. Results: We trained over 275 local safety leaders in ACA methodology, and 148 ACAs were completed during the study period. Most ACAs had moderate potential severity (35.8%), occasional frequency (40.5%), and lowest risk modified SAC score (63.5%)[Table1]. There were 247 actions identified: most resulting in communication/education (41.3%), care process changes (24.3%), and human factors redesign (13.4%). From these ACAs 31 safety stories and 14 Enterprise Safety Bulletins were developed. Association of patient safety culture indicators with unit-based ACAs was analyzed, Culture of Safety Index (p=0.90) and Patient Safety Rating (p=0.51) did not show a significant association, while near-miss safety reporting ratio is associated with ACA performance (p=0.03)[Table 2].
Conclusion(s): ACA Program development with sharing of learnings from near-miss safety incidents supports proactive safety culture. Units with a higher proportion of near-miss safety incident reporting performed more ACAs suggesting a culture that encourages learning before harm occurs is essential to improving patient care.
Figure 1. Modified Safety Assessment Code matrix for determining potential severity and frequency of an event
Table 1. Description of ACAs Performed
Table 2. Relationship of patient safety indicators to ACAs performed for inpatient and ICU clinical care locations in 2022-2024