Medical Student Research Fellow Akron Children's Hospital Akron, Ohio, United States
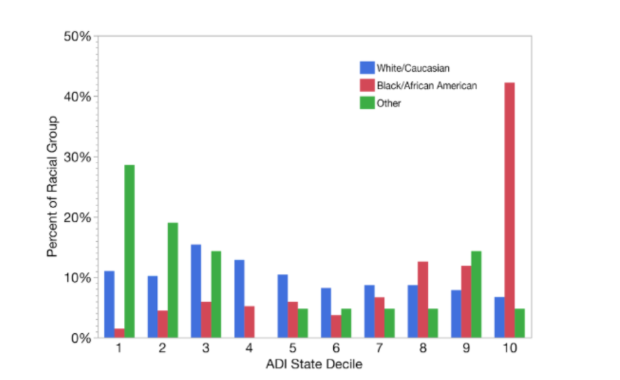
Background: Area Deprivation Index (ADI) is a validated method of evaluating inequalities based off 17 measures of deprivation. At our institution, we had anecdotal concerns about patients with poor socioeconomic status and also racial minorities presenting frequently with surgical magnitude curves (≥45°) when being evaluated for Adolescent Idiopathic Scoliosis (AIS). Objective: The aim of this study was to evaluate demographic differences in patients referred for AIS evaluation and potential disparities in treatment. Design/Methods: All patients referred to a large volume, tertiary Pediatric Spine Center from 2022-2024 for AIS evaluation were reviewed retrospectively. Demographic data, including age, race, ethnicity, gender, insurance type, and address were obtained. Treatment ordered (brace or surgical scheduling) at the time of visit was reviewed. ADI was found using patient addresses. Results: One thousand sixty-seven patients were reviewed, who were predominantly female (65%), English speaking (99%), with a median age of 13 years. The racial composition was largely White/Caucasian (82%), Black/African American (13%), and of non-Hispanic/Latino ethnicity (93%). Race and ADI were statistically significant predictors of a surgical magnitude curve (≥45°) in the model (p < 0.001). Black/African American patients were more likely to require surgery when compared to white patients (OR = 4.5; 95% CI: 2.0, 10.3), or patients of other races (OR = 4.7 (95% CI: 2.0, 10.6). Higher (more deprived) ADI state deciles were associated with a greater likelihood of a surgical magnitude curve (OR 1.34 per 10th percentile increase). There was a trend towards greater likelihood for surgery in patients with government insurance versus commercial (4.0% vs 1.2%, p=0.056). There were no statistically significant differences with surgical scheduling or brace ordering by sex, ethnicity, language, or insurance type, or between brace ordering and race. Black/African American patients were more likely to have socioeconomic deprivation compared to white patients (state decile 9 vs 5, p< 0.001; image 1).
Conclusion(s): African American race and worse socioeconomic status are associated with higher incidence of presentation with a surgical magnitude curve in patients referred for evaluation of AIS. This suggests that late detection of AIS is associated with socioeconomic disparities, likely secondary to limited access to healthcare. Targeted scoliosis screening interventions in areas with a high African American population and/or low socioeconomic status may prove beneficial for earlier detection and implementation of nonsurgical AIS management.

 photo")