107 - Implementation of a Pilot Nasogastric Tube Home Discharge Program in a level IV NICU
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3102.107
Bipashna Malla, St. Christopher's Hospital for Children, Philadelphia, PA, United States; Michael J. Daubert, Drexel University College of Medicine, Philadelphia, PA, United States; Narden Gorgy, St. Christopher's Hospital for Children, Philadelphia, PA, United States; Swosti Joshi, Drexel University College of Medicine/St. Christophers hospital for Children, Philadelphia, PA, PA, United States; Ogechukwu Menkiti, St Christopher's Hospital for Children, cherry hill, NJ, United States; Vilmaris Quinones Cardona, Drexel University College of Medicine, Philadelphia, PA, United States
Neonatal Fellow St. Christopher's Hospital for Children Philadelphia, Pennsylvania, United States
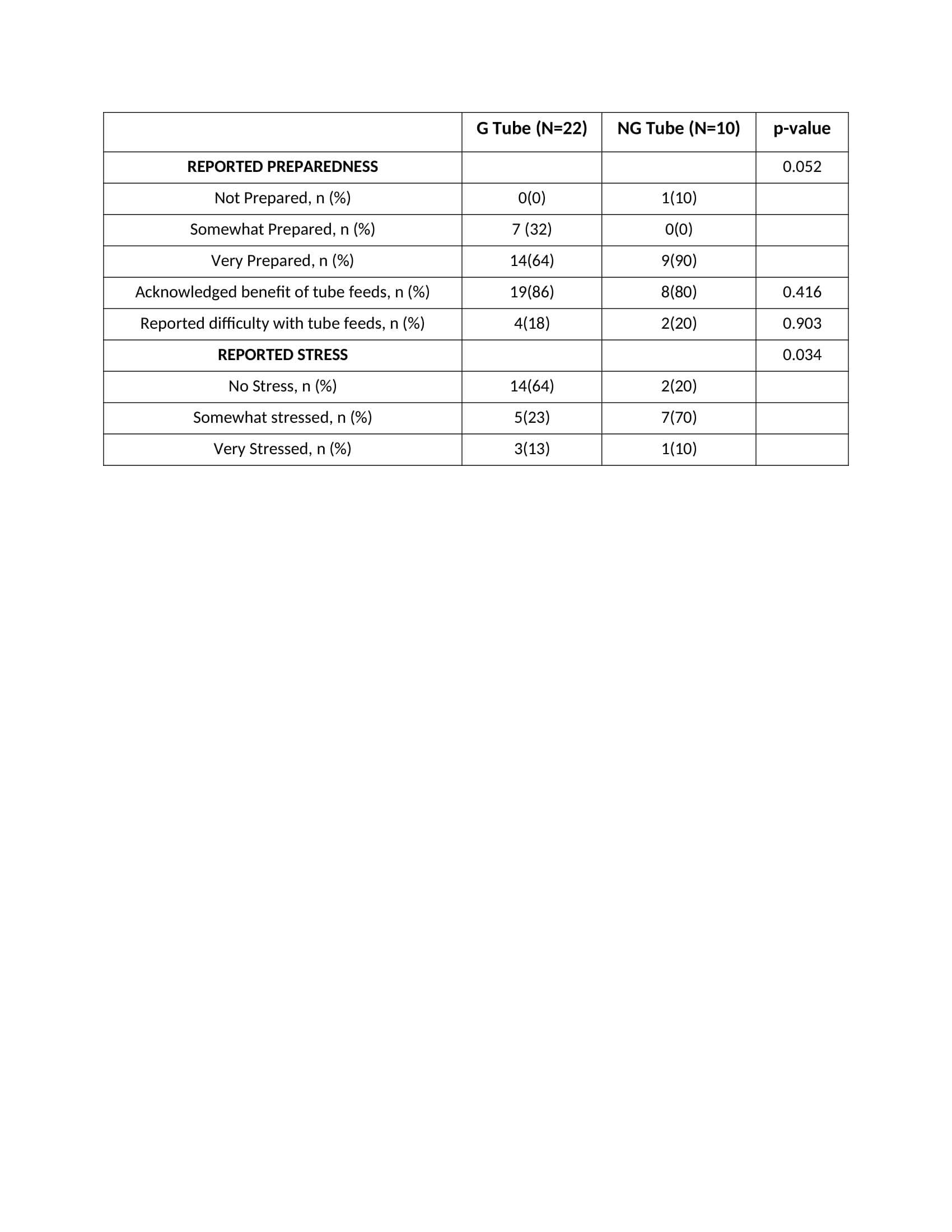
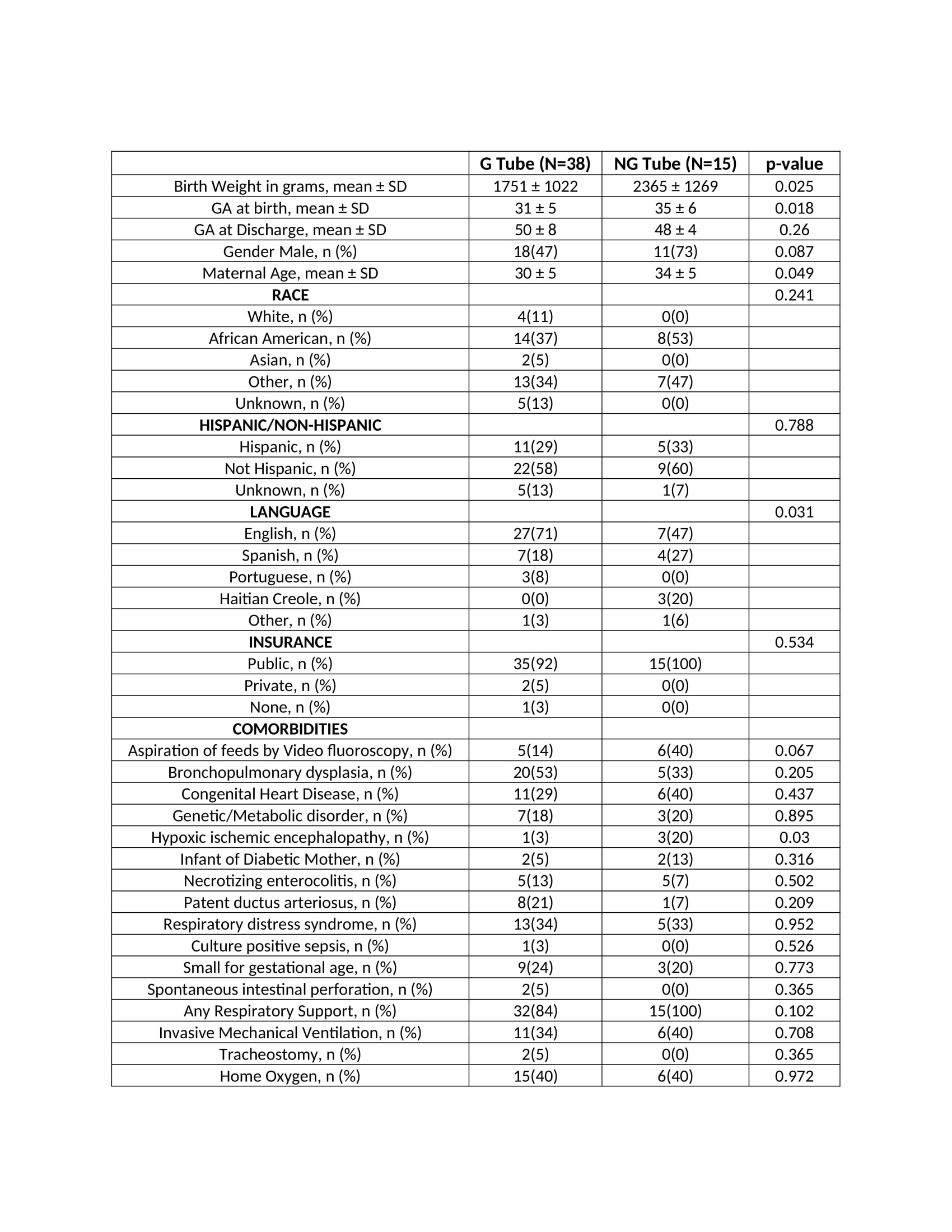
Background: Feeding difficulties affect 80% of premature infants. Most attain full oral (PO) feeds by term, but some need tube support at discharge. Gastrostomy tube (GT) provides long-term support but is associated with higher complication rates, emergency department (ED) visits, and longer length of stay (LOS) than nasogastric tube (NGT). About 70% of infants discharged on NGT achieve full PO feeds by 6 months. In 2025, we launched a pilot home NGT program in our level IV NICU. Objective: To evaluate the short-term outcomes and caregiver satisfaction of infants discharged on NGT and GT feeds. Design/Methods: Retrospective chart review of infants discharged home with NGT and GT from an academic level IV NICU between January 2024 and July 2025. Maternal and neonatal demographics, feeding outcomes, LOS, ED visits, tube-related complications, and time to full PO feeds were collected. A post-discharge caregiver survey assessing satisfaction and complications encountered was administered by phone in the caregivers' preferred language using Voyce interpreting services. Statistical analyses were performed to compare the NGT and GT groups. Results: A total of 53 infants were discharged on tube feedings: 15 (28%) on NGT and 38 (72%) on GT. Neonates discharged with NGT were of a later gestational age than the GT group (35 ± 6 weeks vs. 31 ± 5 weeks, p = 0.018, Table 1). The NGT group had a shorter LOS (68 ± 40 days vs. 100 ± 67 days, p = 0.037; Table 2), and discharge was quicker after the tube-feeding decision (14 ± 12 days vs. 43 ± 57 days, p = 0.006; Table 2) compared to GT group. There was no difference in time to achieve full PO feeds, ED visits, or tube-related complications between groups (Table 2). At 6 months, 60% (9/15) of infants in the NGT group and 21% (7/33) in the GT group achieved full PO feeds. Six infants (40%) in the NGT group required GT placement. While more caregivers in the NGT group felt very prepared to manage home tube feeds, they also reported more stress than those in the GT group (Table 3). The most commonly reported stressor was concern for NGT dislodgement.
Conclusion(s): Implementation of an NGT discharge program in a complex level IV NICU population is safe and feasible. Discharge home on NGT feeds offers a suitable alternative to surgical GT placement, without increasing the burden of ED visits or tube-related complications. Next steps include an educational NICU campaign to share program outcomes, proactively identify patients who can benefit from home NGT feeds to avoid surgery, and developing strategies to mitigate caregiver stress.

 Credit")
.jpg)