339 - Quality improvement project to reduce the frequency of necrotizing enterocolitis stage II or greater in a level III hospital
Sunday, April 26, 2026
9:30am - 11:30am ET
Publication Number: 3326.339
Sujir P. Nayak, UTSW -Dallas, Dallas, TX, United States; Luc P. Brion, UT Southwestern Medical Center, FRISCO, TX, United States; Dimitrios Angelis, University of Texas Southwestern Medical School, Dallas, TX, United States; Mambarambath A.. Jaleel, University of Texas Southwestern Medical School, Irving, TX, United States; Audrey Edwards, Parkland Health, Dallas, TX, United States; Cheryl Lair, University of Texas Southwestern Medical School, Dallas, TX, United States; Steven Brown, Parkland Health, Dallas, TX, United States
Assistant Professor of Pediatrics UTSW -Dallas Dallas, Texas, United States
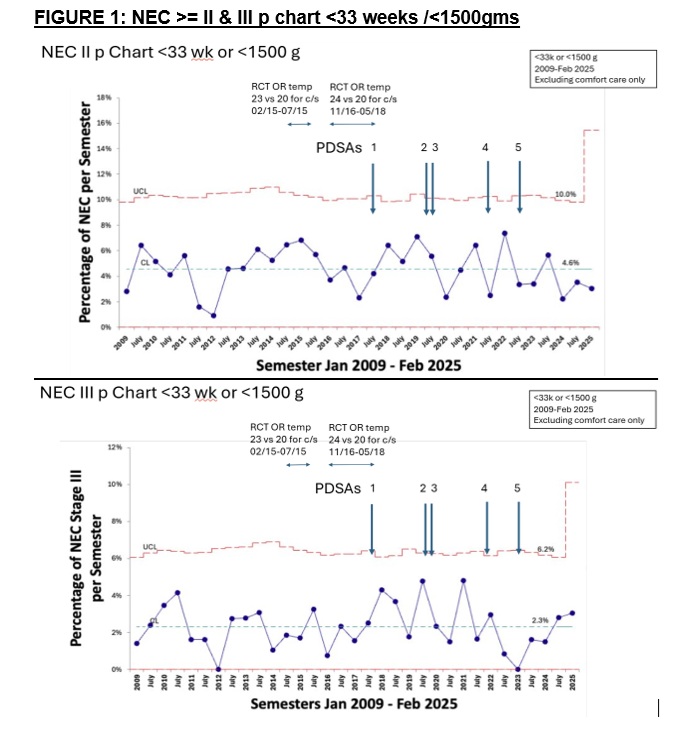
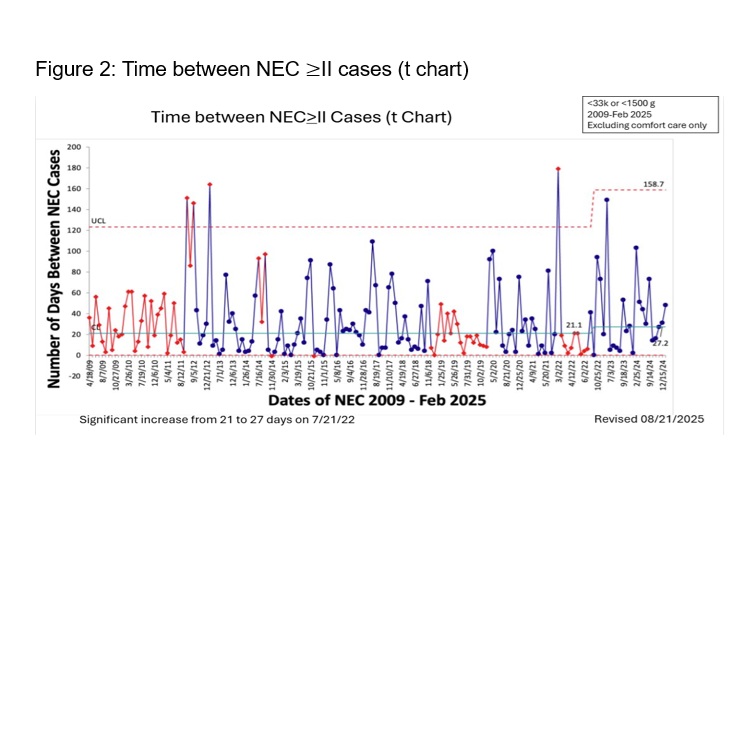
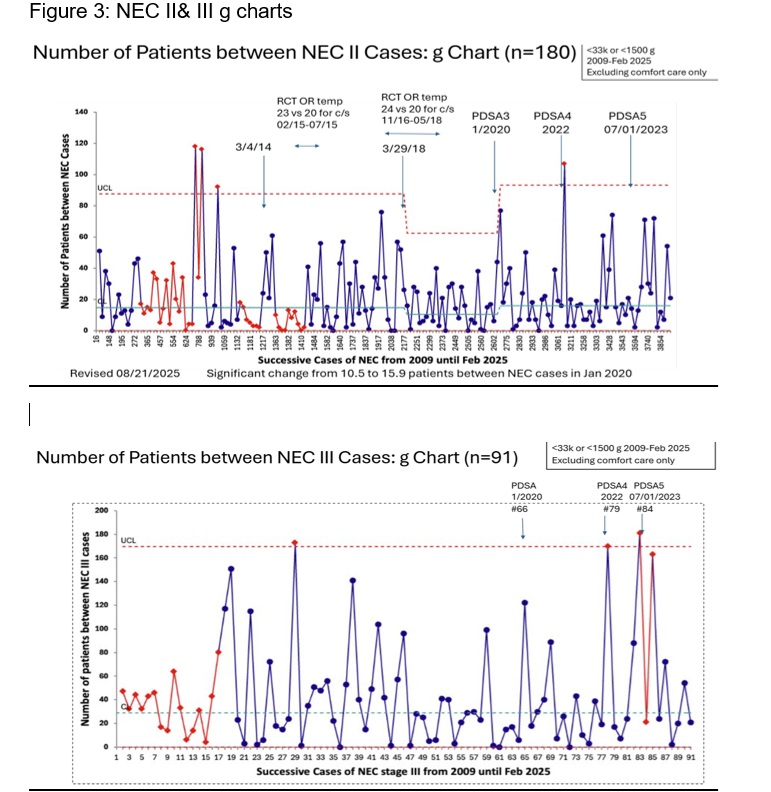
Background: Necrotizing enterocolitis (NEC) is the most common gastrointestinal emergency of very low birth weight (VLBW), preterm infants with a high mortality rate and a high impact on growth and neurodevelopment amongst survivors. A quality improvement project was established in 2018 and went through 5 Plan-Do-Study-Act (PDSA) cycles to decrease NEC stages II and III. Objective: To reduce NEC stage ≥ II among VLBW infants and/or ≤ 32 weeks' gestational age (GA) admitted to Parkland NICU by 20% (from 5.5 to 4.5%) from August 2018 to June 2024 Design/Methods: A key driver diagram was used to find areas to target in our project. The first PDSA cycle (PDSA-1) included increasing administration of mother's own milk (MoM) by education and increasing availability and distribution of pumps before and at delivery. PDSA-2 included encouraging pumping as soon as possible and increasing transportation of maternal own milk (MoM) to the NICU. PDSA-3 included implementation of a donor breastmilk (DBM) program with written parental consent and pneumatic tubing of MoM. PDSA-4 included fresh MoM, meeting nutritional requirements for zinc, and delaying initiation of formula until at least 34 weeks postmenstrual age (PMA). PDSA-5 included increasing efforts to increase MoM production and to prolong MoM as long as possible, early fortification of feeds and limitation in using antibiotics. Statistical Process Control included p charts, t charts and g charts % feeding MoM at discharge were used as balancing measures Results: Among 2598 infants admitted from January 2014 until June 2024, the frequency of NEC ≥II or III did not improve with the project (Figure 1). However, t-charts and g-charts showed points outside the upper control limit and significant increases from 10.5 to 15.9 patients (Figure 2) and from 21 to 27 days between NEC ≥II cases, and from 28 to 91 patients between NEC III cases (Figure 3). The % infants receiving DBM increased from 0-5% in 2016-2019 to 72% in 2020 and 88% in 2021. % of infants in whom formula was delayed until 34 weeks PMA increased from 16% to 89 %. In 2021 the % of infants feeding MoM at discharge significantly decreased.
Conclusion(s): Although the incidence of NEC did not decrease, the time and number of admissions between NEC cases increased significantly after DBM implementation. This data is consistent with importance of t-charts and g-charts in analyzing rare events. Further PDSA cycles will aim at starting DBM on the first day of life and optimize the volume of MoM feeding
figure 1: NEC II & III p Chart <33weeks & <1500 gms
Fig 2: Time between NEC II or greater cases ( t-chart)

 Credit")